Effectiveness of active video games in overweight and obese adolescents: a systematic review and meta-analysis of randomized controlled trials
Article information

Abstract
Purpose
The purpose of this review was to assess the effect of active video games among overweight and obese adolescents.
Methods
A systematic review and meta-analysis were conducted using records from the English-language electronic databases MEDLINE, the Web of Science, and PubMed. These databases were searched from January 2010 to December 2020 using the keywords (adolescent*) AND (overweight OR obese *) AND (active video games OR exergaming * OR video game*).
Results
Five articles met the inclusion criteria. Four studies were conducted in the United States of America and 1 study was conducted in Canada. In addition, all included articles had a randomized controlled trial study design. It was determined that the sample size of the studies was 30–46 participants and there were a total of 195 overweight and obese adolescents across the included studies. Active video gaming was negatively associated with changes in body mass index percentile (mean difference [MD], -1.77; 95% confidence interval [CI], -2.55 to -0.99; P<0.001) and total cholesterol (MD, -11.16; 95% CI, -16.64 to -5.68; P<0.001).
Conclusions
Playing active video games can reduce both the body mass index percentile and total cholesterol in overweight and obese adolescents. Active video games can provide a different method for combating childhood obesity. High-quality randomized controlled trials are recommended to assess the impact of game-based interventions.
Highlights
· Active video games are an effective nonpharmacological practice in reduced body mass index.
· Active video games can be effective in lowering the total cholesterol level.
· Active video games should not be viewed as a independent attempt to reduce weight loss in obese adolescents.
Introduction
Childhood overweightness and obesity are important global public health problems [1]. World Health Organization reports that 340 million children aged 5–19 years were overweight or obese in 2016 [2]. For this reason, the World Health Organization states that physical activity is an important strategy in the fight against obesity in children [3].
Active video games (AVGs), which have been increasingly used by children in recent years, are new-generation games that support increased physical activity and a reduced sedentary lifestyle in children [4]. AVGs increase the energy children spend playing video games and enable them to be more physically active in physical education classes at school or home [5]. In their systematic review, Biddiss and Irwin stated that children who play AVGs have a moderate level of physical activity and suggested that such games have the potential to overcome the obstacles to physical activity. AVGs help increase physical activity motivation in children and adolescents. In this respect, it is seen as a promising alternative to traditional games [6].
There are many studies in the literature examining the effects of AVGs on physical activity, energy expenditure, and anthropometric parameters [7-11]. There are also studies showing that the anthropometric parameters of children who play AVGs improve [5]. Santos et al. [12] reported in their systematic review that AVGs had a positive effect on weight loss and body mass index (BMI). Hernández-Jiménez et al. stated in their systematic review and meta-analysis that the BMI values of children who played AVGs were lower than those of children in the intervention group [13].
It is important to synthesize research findings so that AVGs are very popular among young people, and additional studies can provide useful suggestions for determining the effect of AVGs on weight loss as part of the fight against obesity. The aim of this study was to review the scientific evidence on the effects of AVGs in overweight and obese adolescents.
Materials and methods
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement [14]. In this study, screening, data extraction, selection of studies, and quality evaluation processes were carried out by the first and second authors together in a joint session to reduce the risk of possible errors.
1. Search methods
This study was conducted between January and April 2020 by screening English-language electronic literature databases.
MEDLINE, the Web of Science, and PubMed were systematically reviewed using the following keywords: (adolescent*) AND (overweight OR obese*) AND (active video games OR exergaming* OR video game*).
The reference lists of articles included in this study were checked for additional relevant studies.
The PICOS (population, intervention, comparison, outcomes, and study) framework was used to indicate the clinical questions (Table 1).
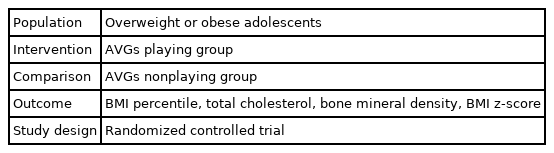
PICOS framework
2. Inclusion and exclusion criteria
Studies needed to adopt the following criteria to be eligible for inclusion:
(1) Focused on overweight or obese adolescents aged 10–19 years;
(2) Were randomized controlled trials (RCTs)
(3) Were published in English between January 2010 and January 2020; and
(4) Examined the impact of AVGs.
The exclusion criteria were as follows:
(1) Study participants had a history of chronic, genetic, or congenital disease;
(2) Studies offered insufficient data on the effect of AVGs on overweightness/obesity; and
(3) Studies did not focus on the effect of AVGs on overweightness/obesity.
3. Data extraction and bias risk assessment of included studies
Two authors independently extracted data into a data-collection form; while 1 researcher (ZEE) extracted data, the other researcher (SÇ) checked them. A data-extraction form was used to systematically extract data related to country/author/year, sample characteristics, type of research, intervention, and outcome of each study.
Five studies described the random sequence generation process [7-10]. Two studies reported information about allocation concealment [10,11]. Inadequate information on allocation concealment or randomization may increase the risk of bias. Three studies described the blinding of the outcome assessors [8,10,11]. Two studies did not clearly report the incomplete outcome data [8,10]. Three studies (60%) reported a low risk for selective reporting [7,9,11] and 2 studies (40%) reported a low risk of bias for other types of bias [7,11].
4. Statistical analysis
Adolescents' results of BMI percentile, BMI z-score, cholesterol, and spine bone mineral density were combined by meta-analysis.
Three studies measuring postintervention BMI percentile [7,9,11], 2 studies measuring postintervention BMI z-score [10,11], 2 studies measuring postintervention total cholesterol [10,11], and 2 studies measuring postintervention bone mineral density [10,11] were included in the meta-analysis.
All analyses were conducted using Review Manager (version 5; Cochrane, London, UK). For continuous variables of RCTs, the mean difference (MD) at a confidence interval (CI) of 95% was used. The standardized MD was calculated for the continuous variable. If I2<50%, then a fixed-effects model was used; otherwise, a random-effects model was used. All tests were calculated from a 2-tailed test, and P<0.05 was considered to be statistically significant.
Results
1. Results of the literature search
A total of 1,737 records were identified from the aforementioned databases and 6 records were collected from other sources. After removing 720 duplicate articles, the titles and abstracts of 1,023 articles were screened and an additional 451 records were excluded. The full-text versions of 572 articles were then screened and 5 RCTs were finally included in the qualitative synthesis. Fig. 1 shows the PRISMA flow diagram of the search process.
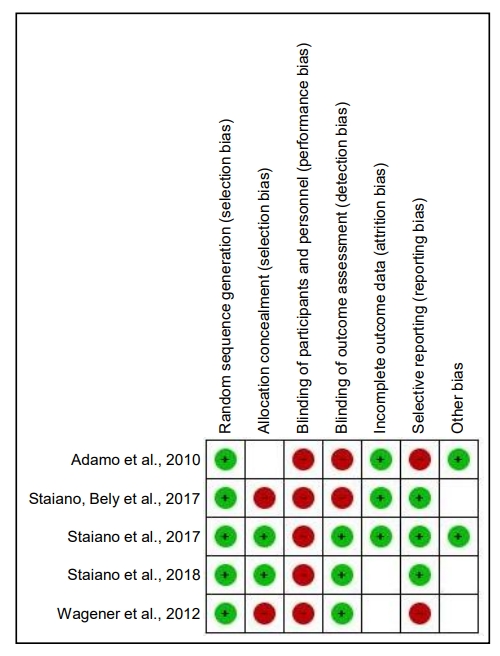
Risk of bias of 5 studies according to the Cochrane Handbook for Systematic Reviews of Interventions (“+” means low risk; “−” means high risk; “?” means unclear risk).
2. Quality assessment
Two authors (ZEE and SÇ) assessed the quality of the studies based on the JBI Critical Appraisal Checklist for RCTs [15]. Two researchers independently evaluated the risk of bias. The risk of bias among the RCTs was assessed according to the Cochrane Handbook for Systematic Reviews of Interventions [16]. Fig. 2 presents the risk of bias and Table 2 summarizes the methodological quality assessment.
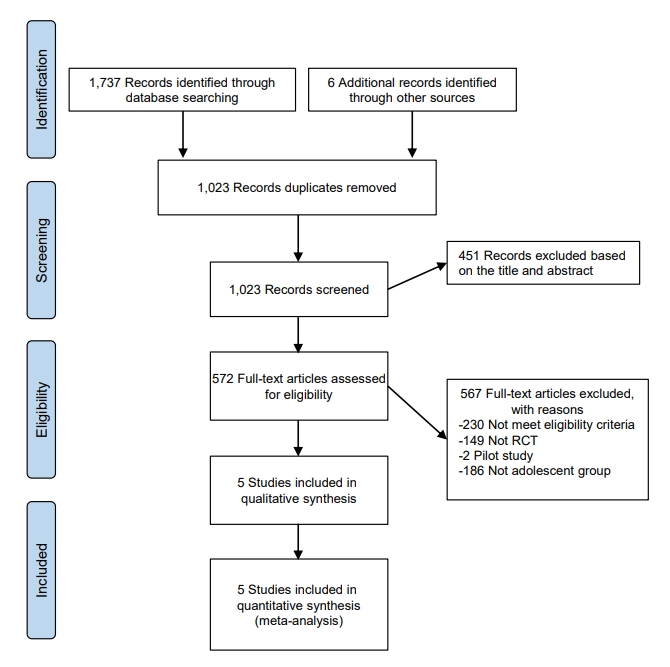
PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) flow diagram of the search process. RCT, randomized controlled trial.

Methodological quality assessment of 5 studies according to the Randomized Controlled Trial Checklist of Joanna Briggs Institute
3. Characteristics of the included studies
Five articles were published from 2010–2020. Four studies were conducted in the United States of America and 1 study was conducted in Canada. All articles (n=5) were written in English. Also, all included articles had an RCT study design. It was determined that the sample size of the studies ranged from 30–46 participants, and there were a total of 195 overweight and obese adolescents across all the studies (Table 3).

Characteristics of the studies
1) BMI percentile
Three studies measured the effect of AVGs on BMI percentile [7,9,11]. The pooled result reports that AVG interventions led to a significant reduction in BMI percentile in the intervention group (MD, -1.77; 95% CI, -2.55 to -0.99; P<0.001) (Fig. 3).
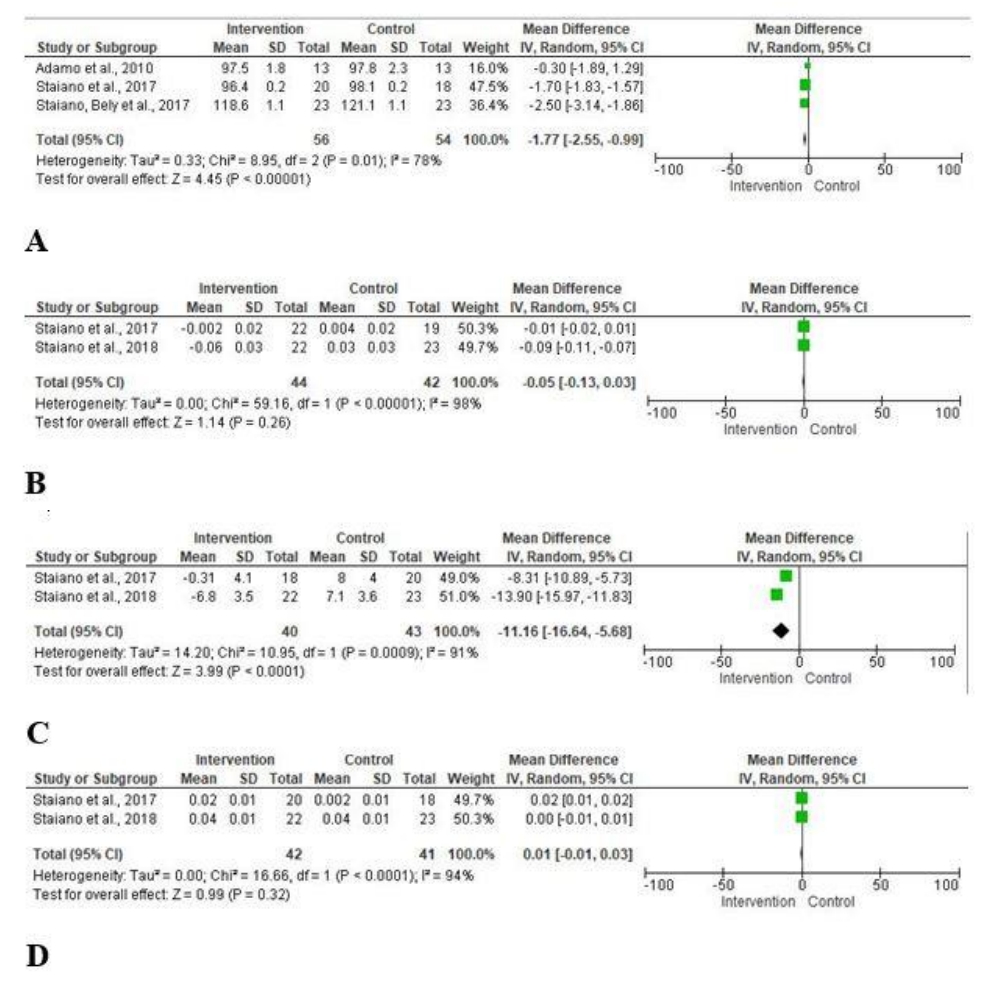
Meta-analysis and forest plots for the effect of active video games in overweight and obese adolescents. (A) Body mass index (BMI) percentile. (B) BMI z-score. (C) Total cholesterol. (D) Bone mineral density. SD, standard deviation; CI, confidence interval; df, degrees of freedom.
2) BMI z-score
Two studies measured the effect of AVGs on BMI z-score after intervention [10,11]. No significant difference was found in BMI z-scores between groups (MD, -0.05; 95% CI, -0.13 to 0.03; P>0.05) (Fig. 3).
Discussion
This review provides an overview of what is known about the effect of AVGs in overweight and obese adolescents. The strength of this study is that each parameter was evaluated within itself. Also, only RCTs were included.
Reductions in physical activity, changes in eating habits, and an increase in the use of digital tools contribute to childhood obesity [1]. AVGs require full-body participation, unlike traditional video games. In addition, it is an important advantage that games allow participation of the whole family and can be played at home and for combating childhood obesity [17].
Within the scope of a systematic review and meta-analysis, it was found that overweight and obese adolescents who played AVGs had a lower BMI percentile. However, it was also found that AVGs had no effect on BMI z-score. Likewise, in a systematic review, Zeng and Gao [16] reported that the use of exergames in 4 out of 7 RCTs decreased the BMIs of participants. Unlike in the present study, however, in a systematic review by Gao and Chen [17], the use of exergames had no effect on BMI. These studies showed that BMI percentile and BMI z-score are not calculated separately. The BMI z-score shows how much deviation exists from the data of the general population. The lack of significant change in the BMI z-score is thought to be due to the fact that it was calculated according to age and gender [18]. It was also reported that BMI z-score is a weak measure for determining changes in total body fat [19].
Meta-analysis results are very important in terms of guiding future studies. Most of the RCTs discussed herein were carried out for 10–12 weeks. Only Staiano et al. [10] conducted a 24-week study. They stated that the BMI z-score of adolescents who played exergames decreased. Monitoring in RCTs for a longer period would enable investigators to see the effects of interventions on anthropometric measurements better.
In the studies reviewed, it was found that obese and overweight adolescents who actively played video games experienced a decrease in their total cholesterol level. It is thought that AVGs can be effective in lowering the total cholesterol level.
Within the scope of the systematic review and meta-analysis, it was found that AVGs had no effect on the bone mineral density of obese and overweight adolescents.
There were only 2 RCTs that examined the effect of AVGs on total cholesterol and bone mineral density. Thus, more studies are needed to determine the effect of AVGs on total cholesterol and bone mineral density.
The present study has some limitations. The first limitation is that we studied only patients in the adolescent age group, which enabled us to retrieve a limited number of studies. The second limitation is that we were restricted to obtaining a cumulative result since we considered BMI as a percentile and BMI z-score separately. The third limitation is that the number of RCTs examining total cholesterol and bone mineral density was quite limited. Finally, since studies examining the effect of AVGs on obesity in adolescents are limited in number, the frequency and duration of the games played and the devices used vary in the studies discussed.
In conclusion, this report of a systematic review and meta-analysis gives an overview about the relationship between overweightness and obesity and AVGs. The identification of this relationship can yield a different method for combating childhood obesity. This study concluded that AVGs were effective in reducing the BMI percentile and total cholesterol level but not in improving the BMI z-score or bone mineral density. Although the integration of allocation concealment, research design, and sample size needs to be improved, our findings are promising for promoting physical activity using AVGs. AVGs may be integrated into schools and homes. Encouraging physical activity via AVGs can be successful in the fight against obesity.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data availability
The data that support the findings of this study can be provided by the corresponding author upon reasonable request.
Author contribution
Conceptualization: ZEE, SC; Formal analysis: ZEE; Methodology: ZEE, SC; Writing - original draft: ZEE; Writing - review & editing: SC