Factors affecting height velocity in normal prepubertal children
Article information

Abstract
Purpose
To analyze the effects of clinical and laboratory factors, including insulin-like growth factor (IGF) levels, on the height velocity of normal prepubertal children.
Methods
Ninety-five healthy prepubertal children (33 boys, 62 girls) were enrolled. The mean chronological age was 6.3±1.4 years, with a height standard deviation score (SDS) of -0.88±0.70. IGF-1, IGF binding protein-3 (IGFBP-3), SDS for anthropometric measurements, and changes in SDS for anthropometric measurements were analyzed for 1 year, and their associations with 1-year height velocity were investigated.
Results
The group of children with a 1-year height velocity of ≥6 cm were chronologically younger than the group with a 1-year height velocity of <6 cm (5.9±1.3 years vs. 6.7±1.3 years, P=0.004), with a lesser increase of SDS for body mass index (BMI) over 1 year (-0.18±0.68 vs. 0.13±0.53, P=0.014). There were no differences between the 2 groups in IGF-1 SDS and IGFBP-3 SDS. Multiple linear regression showed that baseline chronological age (r=0.243, P=0.026) and height SDS (r=0.236, P=0.030) were positively associated with IGF-1 SDS. Binomial logistic regression showed that an older chronologic age at referral (odds ratio [OR], 0.68; 95% confidence interval [CI], 0.47–0.99) and an increase of BMI SDS over 1 year (OR, 0.41; 95% CI, 0.18–0.89) were associated with a decreased growth possibility of an above-average height velocity (≥6 cm/yr).
Conclusions
Height velocity of normal prepubertal children is affected by an increase of BMI SDS and chronological age. Prepubertal IGF-1 SDS reflects height SDS at the time of measurement but is not associated with subsequent height velocity.
Introduction
Human growth is affected by complex interactions among various factors, including gene, race, birth weight, hormone, nutrition, and environment [1-6]. In children, height growth may be divided into 3 periods: first 2 years of life, prepuberty, and puberty [7]. During the first 2 years of life, height velocity, and weight gain rapidly decreases. Before puberty, growth rate is relatively slow, where boys and girls alike grow by about 5–6 cm a year with an average of 2.5-kg weight gain annually [8]. Diverse factors, such as exercise, sleep, and nutrition, affect the height velocity of prepubertal children. Exercise helps height growth by increasing the secretion of growth hormones (GHs) [9]. Sufficient sleep may prevent obesity and stimulates the release of GHs, thereby affecting height growth [10]. A balanced diet is an essential factor of growth [11]. The number of overweight and obese children has increased worldwide in recent years, which has facilitated growth rates of prepubertal children and has affected the onset of puberty as well [12-15].
GH and insulin-like growth factor (IGF) play an important role in regulating height growth [16]. IGF binding protein (IGFBP) transports and increases the half-life of IGF while helping free IGF in blood to bind to IGF receptors, ultimately promoting growth [17-19]. IGF-1 helps the diagnosis of GH deficiency and is used for evaluating growth during GH therapy [20,21]. IGF-1 is associated with height growth in early childhood. It elevates in advancing age, reaching a peak concentration in Tanner stages III–IV during puberty, a period marked by explosive growth, after which it declines [22-24].
The authors aimed to identify the clinical and biochemical factors that affect height velocity in prepubertal children and to investigate the clinical relevance of IGF-1 in prepubertal growth.
Materials and methods
1. Subjects
Ninety-five healthy prepubertal children (33 boys and 62 girls) who visited the pediatrics department at Catholic University Yeouido St. Mary’s Hospital between January 2009 and June 2016 for growth evaluation were enrolled.
Children with an endocrine disease, chromosomal disease, chronic disease, or small for gestational age, or of short stature (height below 2 standard deviation scores [SDS]) were excluded from the study.
The chronological age and bone age of the participants were 6.3±1.4 years and 5.4±1.7 years, respectively, and the children's birth weight and gestational age were 3.2±0.5 kg and 38.8±1.8 weeks, respectively. The midparental height (MPH) SDS was -0.40±0.59, and height SDS was -0.88±0.70. The body weight SDS was -0.69±1.04, and body mass index (BMI) SDS was -0.18±1.07. The IGF-1 SDS was -0.26±0.94 and IGFBP-3 SDS was -0.33±1.15 (Table 1).
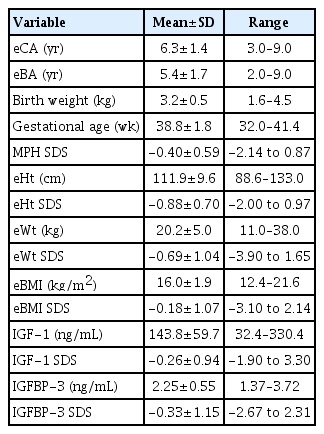
Descriptive characteristics of normal prepubertal children at baseline (n=95)
2. Method
Height was measured to the 0.1 cm using a Harpenden Stadiometer (Holtain Ltd., Crymych, UK). Three measurements were taken, and the average was used for analysis. Bone age was measured by taking plain radiographs of the left hand and wrist and using the Greulich-Pyle method. The average of the measurements taken by 1 radiologist and 2 pediatric endocrinologists was used for analysis. For MPH, 6.5 cm was added to (boys) or subtracted from (girls) to include the average of the parents’ heights. BMI was computed using the following formula weight (kg)/[height (m)]2. SDS of height, weight, BMI, and MPH were taken from the 2007 Korean Children Growth Chart [17]. Sexual maturity was rated according to the Marshall-Tanner method [18]. Serum IGF-1 and IGFBP-3 were measured using the RIA kit (Automatic Gamma-10 counter, Shinjin Medix, Goyang, Korea). The SDS for IGF-1 and IGFBP-3 were taken from the corresponding reference values given in the 2012 data from Korean children and adolescents [19]. Thyroid function was measured with the radioimmunoassay test (TSH IRMA Kit, fT4 RIA kit, SR300, Usti nad Orlici, Czech Republic).
At the initial visit, the participants’ height, weight, sexual maturity, bone age, thyroid function test, IGF-1, and IGFBP-3 were measured, and height, weight, sexual maturity, and bone age were again measured 1 year later. Height velocity over the year (cm/yr) was computed to analyze its associations with birth weight, gestational age, chronological age, bone age, height, weight, BMI, MPH, IGF-1, and IGFBP-3.
This study was approved by the Institutional Review Board of Yeouido St. Mary’s Hospital (approval number: SC17RESI0047). Written informed consent by the patients was waived due to a retrospective nature of our study.
3. Statistics
Measurements and calculations were presented as mean±standard deviation. Statistical analysis was performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). Changes in height, weight, and BMI over 1 year were analyzed using the paired t-test, and associations of height velocity with other variables were analyzed with the Student t-test. The effects of each variable on height velocity were examined using multiple linear regression and multiple logistic regression. Data with P<0.05 were deemed statistically significant.
Results
1. Comparison of clinical and laboratory parameters in relation to height velocity
Height SDS significantly increased from -0.88±0.70 to -0.79±0.71 after 1 year (P=0.001), and weight SDS significantly increased from -0.69±1.04 to -0.42±1.02 (P=0.001). BMI SDS did not differ (-0.18±1.07 to -0.19±1.05) (P=0.904) (Fig. 1). The participants' mean height growth over 1 year was 6.1±1.3 cm/yr.
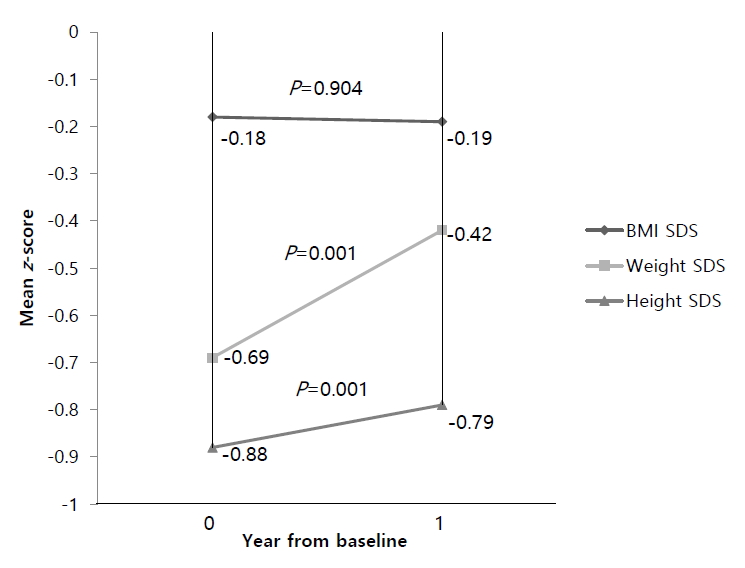
Body mass index (BMI), weight and height standard deviation score (SDS) changes over 1 year.
Forty-three participants (45%) grew by more than 6 cm over the year, while 52 participants (55%) grew by less than 6 cm. In comparison of the clinical and laboratory parameters between the 2 groups, the ≥6 cm growth group was chronologically younger than the <6 cm group (5.9±1.3 years vs. 6.7±1.3 years, P=0.004) (Table 2), had a younger bone age (4.9±1.6 years vs. 5.8±1.6 years, P=0.006) (Table 2), and lesser increase of BMI SDS over 1 year (-0.18±0.68 vs. 0.13±0.53, P=0.014) (Table 2).

Clinical and laboratory parameters of normal prepubertal children according to height velocity for 1 year
There were no significant differences between the ≥6 cm growth and <6 cm growth groups in IGF-1 SDS (-0.20±0.88 vs. -0.31±0.99, P=0.575) (Table 2) and IGFBP-3 SDS (-0.25±1.14 vs. -0.41±1.18, P=0.552) (Table 2).
2. Comparison of clinical and laboratory parameters in relation to IGF-1 SDS, IGFBP-3 SDS
IGF-1 SDS was positively correlated with the baseline chronological age (r=0.342, P=0.001) (Fig. 2) and baseline height SDS (r=0.319, P=0.002) (Fig. 2) but was not associated with changes in height SDS, weight SDS, and BMI SDS over 1 year, and MPH SDS.
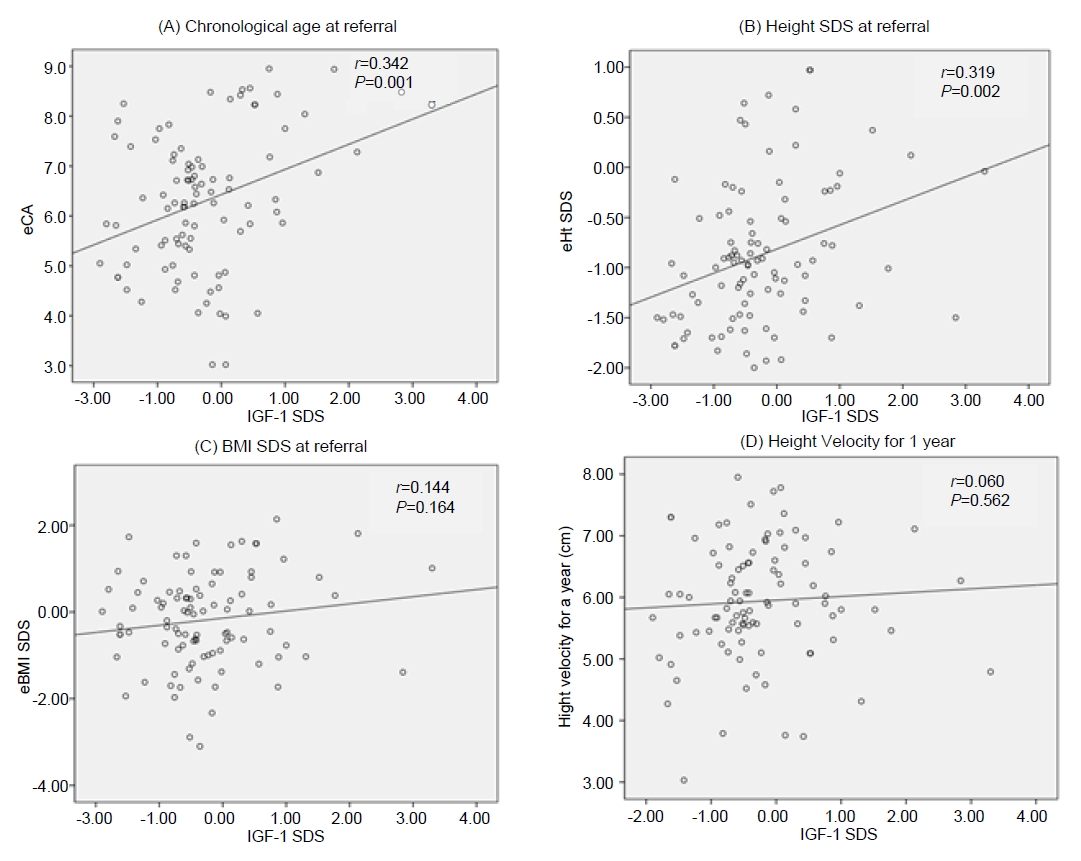
Distribution of clinical parameters according to insulin-like growth factor-1 (IGF-1) standard deviation score (SDS). eCA, chronological age at referral; eWt, weight at referral; eBMI, body mass index at referral.
Multiple linear regression showed that IGF-1 SDS was positively correlated with baseline chronological age (r=0.236, P=0.026) and baseline height SDS (r=0.236, P=0.030) (Table 3).

Multiple linear regression analysis for IGF-1 SDS with factors of normal prepubertal children
IGFBP-3 SDS was not significantly associated with baseline bone age, chronological age, height SDS, BMI SDS, changes of height SDS over 1 year, changes of weight SDS and BMI SDS over 1 year, and MPH SDS.
3. Multiple logistic regression to identify factors that contribute to increasing relative height velocity
To identify clinical and biochemical factors that increase relative height velocity, participants were divided into ≥6 cm growth and <6 cm growth groups and were analyzed with multiple logistic regression. The results showed that an older chronologic age at referral (odds ratio [OR], 0.68; 95% confidence interval [CI], 0.47–0.99; P=0.046) and an increase of BMI SDS over 1 year (OR, 0.41; 95% CI, 0.19–0.89; P=0.025) were associated with a decreased probability of growth with an above-average height velocity (≥6 cm/yr) (Table 4).
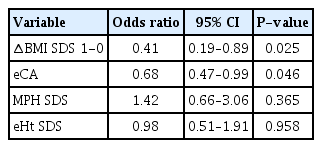
A Multivariable logistic regression model for relatively higher height velocity (≥6 cm/yr) for 1 year of normal prepubertal children
Discussion
In this study, normal prepubertal children with a greater change in BMI SDS had lower height velocity over 1 year. Although the participants included in this study were prepubertal children with normal stature, the findings must be interpreted in consideration of the fact that the standard deviation of height was -0.88, suggesting that they were relatively shorter children. In previous studies, overweight or obesity before puberty was associated with a relative increase of growth [25]. Obese children were taller than children of normal weight during childhood, and obesity during early childhood and childhood was associated with an increase of height throughout childhood [26]. Another study investigating growth reported that a considerable increase of BMI in ages 2–8 was associated with a tall height at age eight [13]. Similar to these findings, our study found that baseline BMI SDS and height SDS were positively correlated. BMI SDS after 1 year of referral and height SDS after 1 year of referral were also positively correlated. These results are in line with previous findings. Based on these results, it can be expected that obese prepubertal children would show an increased growth rate over 1 year, but baseline BMI SDS and height velocity over 1 year were not significantly correlated. On the other hand, changes in BMI SDS over 1 year had a significant negative correlation with height velocity over 1 year, suggesting that an increase of BMI may have an adverse effect on height growth in relatively shorter children. Additional studies are needed to investigate whether the effects of BMI changes on height growth persist for longer than 1 year and whether improving BMI in obese children is helpful to improve height velocity.
Children who were chronologically older showed a slower height velocity over 1 year in our study, and this seems to reflect the normal growth pattern observed among children in the chronological ages of 5–9 years, which was the age group included in our study [27].
MPH is used to assess whether a child's current height percentile matches their genetically anticipated height [10]. Children with a high MPH are at higher odds of reaching a taller final height, so it could be predicted that it would be associated with children’s height velocity over 1 year. However, MPH SDS was not significantly correlated with height velocity for 1 year in our study. Additional studies with longer follow-up periods (>1 year) are needed to examine whether MPH SDS affects long-term height velocity.
Bone age is used for growth assessment and for the prediction of adult height of normal children [28]. Bone age increases with age, and height increases with bone age [29,30]. Few studies have investigated whether a large bone age increase before puberty leads to a greater height growth. In our study, change of bone age over 1 year was not correlated with height velocity in the same year. The fact that the participants were limited to prepubertal children and that the follow-up period to observe changes of bone age was relatively short (1 year) may have contributed to this outcome. As changes in bone age and height velocity may be more significantly associated immediately before or during puberty. Additional studies should be performed to substantiate this.
In our study, IGF-1 SDS and height velocity for 1 year were not associated. Meanwhile, IGF-1 SDS was positively correlated with chronological age at referral as well as with height SDS at referral. IGF-1 SDS is speculated to have a positive correlation with baseline chronological age because the sample showed a significant pattern where height SDS increased with age. On the other hand, IGF-1 SDS was not significantly correlated with BMI SDS at referral. This is in line with a previous finding that obese children and normal weight children do not significantly differ in total IGF-1 concentration [31]. In multiple linear regression, IGF-1 SDS was significantly associated with chronological age and height SDS at referral, suggesting that IGF-1 is an important factor reflecting current growth status.
This study has a few limitations. First, the sample was too small to represent the heights and weights of normal children. Our participants’ heights were generally distributed between -1.5 SDS and 0.5 SDS and weights between -1.5 SDS and 0 SDS. Therefore, the findings of this study have limited generalizability to the entire normal children population, and the results should be interpreted noting that they show the growth patterns in prepubertal children with a relatively short stature. Second, although the participants’ height SDS and weight SDS significantly increased over 1 year, BMI SDS remained largely consistent. This result is not representative of the general changes of height and weight over 1 year in all normal prepubertal children. The fact that participants were educated about lifestyle habits, dietary habits, and sleep habits on their initial visit may have influenced height growth, and more specific analyses are needed to examine this matter. Third, this study was able to confirm that an increase of BMI SDS affects height velocity in the same period, but we could not identify the factors that affect BMI SDS. In the future, studies should analyze the interaction among and the effects of the various factors previously mentioned.
In conclusion, this study found that height velocity in prepubertal children is influenced by an increase of BMI SDS and chronological age. Additionally, prepubertal IGF-1 SDS is a factor reflecting height SDS at the time of measurement but is not associated with height velocity thereafter.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.