The influence of gonadotropin releasing hormone agonist treatment on the body weight and body mass index in girls with idiopathic precocious puberty and early puberty
Article information

Abstract
Purpose
This study aimed to investigate the influence of gonadotropin releasing hormone agonist (GnRHa) treatment on the weight and body mass index (BMI) of girls who were diagnosed with idiopathic central precocious puberty (CPP) or early puberty (EP).
Methods
Patients who were younger than 8 years of age at diagnosis were classified as CPP and patients aged between 8 and 9 years at diagnosis were classified as EP. Of 129 patients, 34 were diagnosed with CPP and 95 were diagnosed with EP. The patients were divided according to pretreatment weight status into normal weight group, an overweight group, or an obese group.
Results
No significant changes were observed with respect to the weight standard deviation score (SDS) before and after 1 year, 2 years of treatment, respectively (P>0.05, P>0.05) in all patient groups. No significant changes were observed in relation to the BMI SDS before and after 1 year, 2 years of treatment, respectively (P>0.05, P>0.05) in all patient group. Depending on the degree of obesity, differences with respect to the weight SDS and BMI SDS were observed.
Conclusion
BMI SDS increased in the GnRHa-treated patients as a whole group, but was not statistically significant. But BMI SDS increased significantly in the normal weight group after 2 years of GnRHa treatment. So, GnRHa treatment may affect the change of BMI SDS depending on degree of obesity.
Introduction
Precocious puberty in girls generally refers to breast development that begins before the age of 8 years, while early puberty (EP) is defined as puberty that occurs between the ages of 8 and 9 years1). Idiopathic central precocious puberty (CPP) occurs because of the early activation of the hypothalamic-pituitary-gonadal axis and it is not associated with any organic abnormalities2). CPP can be diagnosed based on the increase in the luteinizing hormone (LH) concentration that follows the administration of gonadotropin-releasing hormone (GnRH) or a gonadotropin-releasing hormone agonist (GnRHa) once the activation of the hypothalamic-pituitary-gonadal axis has been confirmed. If the LH concentration is higher than 5 IU/L after administration of GnRH, or the ratio between the peak LH concentration and the peak follicle-stimulating hormone (FSH) concentration is greater than or equal to 1.0, a patient is deemed to have reached puberty34). Increases in estrogen secretion in girls may lead to advanced bone aging, reduced final adult heights, early menarche, and various psychological problems.
GnRHa depot injections safely and effectively inhibit the hypothalamic-pituitary-gonadal axis, and they have been widely used since the mid-1980s4). The results from investigations into the influence of GnRHa treatment on weight have been reported by many researchers, but they are inconsistent. Many researchers have reported that GnRHa treatment is associated with weight gain that may persist after treatment and may cause obesity5678910). However, other researchers have reported that GnRHa treatment is not associated with body mass index (BMI) increases11121314). Some studies have reported BMI decreases after GnRHa treatment1516).
This study was conducted to investigate the influence of GnRHa treatment on the body weight and BMI of female patients who were diagnosed with CPP or EP.
Materials and methods
1. Subjects
This study was approved by the Inje University Busan Paik Hospital Institutional Review Board (approval number: 16-166). We retrospectively reviewed the medical records of all of the girls who had been referred to the Division of Pediatric Endocrinology and Metabolism at Inje University Busan Paik Hospital between January 2012 and April 2014, because they had clinical signs of CPP or EP.
Of the female patients who visited the pediatric endocrinology clinics with early pubertal signs, those who met the following criteria were selected for this study: (1) the patient who had reached Tanner breast stage 2 before the age of 8 years, or already had menarche, (2) LH peak >5.0 IU/L in GnRH stimulation test, (3) bone age higher than chronological age by one or more years, (4) the absence of pathologic ovarian lesions based on pelvic sonography. (5) the absence of other diseases that may influence the BMI, and (6) the use of GnRHa treatment for at least 2 years. Patients were excluded from the study if they had endocrine disorders other than precocious puberty, had organic abnormalities including brain lesions, or showed abnormal ovarian, adrenal glands, or thyroid function.
One hundred forty-six girls were screened to participate in this study, and 17 patients were excluded from complete analysis. Exclusion criteria were as follows: subjects who stop GnRHa treatment (n=11), did not perform laboratory tests (n=4), and miss bone age evaluations (n=2) during the follow-up period.
Patients who were younger than 8 years of age at the time of diagnosis were categorized as CPP, and those who were aged between 8 and 9 years at the time of diagnosis were categorized as EP. Of the 129 patients, 34 had CPP and 95 had EP.
2. Methods
The patients' medical records were reviewed retrospectively. The patients' heights, weights, chronological ages, bone ages, and BMIs at the times of the GnRH stimulation tests were recorded. Height was measured to the nearest tenth of a centimeter using a Harpenden stadiometer (Holtain Ltd., Crymych, UK) and weight was measured to the nearest tenth of a kilogram using an electronic scale. The standard deviation scores (SDS) for height, weight, and BMI were calculated using the 2007 Korean National Growth Charts by LMS method17).
Bone age was measured using the Greulich-Pyle method18). During a GnRH stimulation test, the baseline concentrations of LH, FSH, and estradiol were measured, then 100 µg of synthetic GnRH (Relefact, Handok Pharmaceuticals, Seoul, Korea) was injected into the patient intravenously. Subsequently, the concentrations of LH and FSH were measured at 30, 45, and 60 minutes after the injection. The serum LH and FSH concentrations were measured through electrochemiluminescence immunoassay using an Elecsys assay and a eCobas E601 or E602 Kit (Roche Diagnostics GmbH, Mannheim, Germany). The lower detection limits for LH and FSH were 0.100 mIU/mL and <0.100 mIU/mL, respectively.
Pelvic sonography was done on all of the patients, and the results were analyzed by an expert. All of the patients who were younger 8 years of age underwent pituitary magnetic resonance imaging. The BMI was calculated as the body mass (kg)/height (m2), and the corresponding SDS was calculated based on the patient's chronological age and bone age. The patients were grouped based on their body weights and according to their age and sex into a normal weight group (5th–84th percentile), an overweight group (85th–94th percentile) and an obese group (95th percentile and above).
The sexual maturity ratings were determined using the Marshall and Tanner method19). The midparental height was calculated by subtracting 6.5 cm from the parents' mean height20).
Patients who were diagnosed with CPP or EP were administered triptorelin or leuprolide acetate depots injections every 28 days . The doses administered was determined based on the patient's weight: <20 kg, 1/3 vial; ≥20 kg to <30 kg, 2/3 vial; and ≥30 kg, 1 vial (1 vial contained=3.75 mg).
3. Statistical analysis
All of the measurements and calculations are expressed as the means±standard deviations. MedCalc statistical software (ver. 16.4.3, MedCalc Software bvba, Ostend, Belgium) was used for the statistical analyses. Student t-test was used to compare values between CPP and EP groups. A paired t test was used to compare the variables associated with GnRHa treatment. A multiple regression analysis was performed to assess the influence of the variables on the BMI SDS changes. It was determined that statistical significance was attained when P<0.05.
Results
1. Patients' characteristics
The characteristics of the 129 patients who were enrolled to participate in the study are shown in Table 1. The mean chronological age and bone age of the total patient population at the time of diagnosis were 8.49±0.60 and 10.53±0.82 years, respectively. The difference between the bone age and the chronological age was 2.04±0.75 years. The chronological age and the bone age were significantly higher in the patients diagnosed with EP compared with those who diagnosed with CPP. Bone age-chronological age was significantly higher in the patients diagnosed with CPP compared with those who diagnosed with EP.
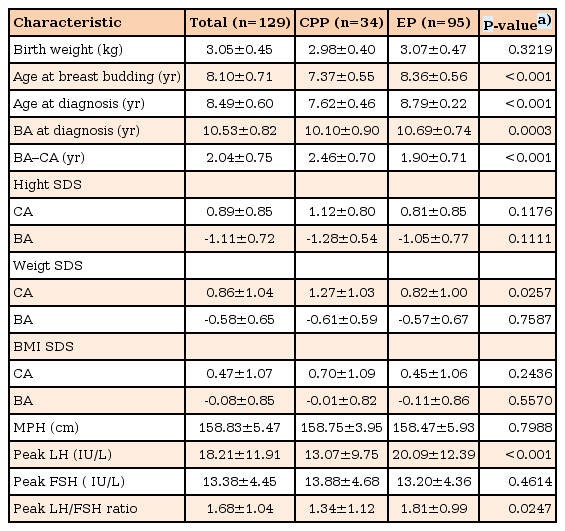
Comparative clinical characteristics of girls with idiopathic central precocious puberty or early puberty
There were no significant differences between the groups with respect to the height SDS based on the chronological age, or the bone age. The weight SDS based on the chronological age was significantly higher in the patients diagnosed with CPP compared with those who diagnosed with EP (P=0.0257). There was no significant difference between the groups with respect to the weight SDS based on the bone age (P>0.05). The mean BMI of the patient population was 17.47±2.21 kg/m2. There was no significant difference between the groups regarding the BMI SDS based on the chronological age (P>0.05).
2. Weight SDS and BMI SDS changes in all patients after GnRHa treatment
The weight SDS was 0.86±1.04 before GnRHa treatment, 0.97±1.00 after 1 year treatment, and 0.81±0.92 after 2 years of GnRHa treatment; No significant changes were observed with respect to the weight SDS (P>0.05, P>0.05). The BMI SDS was 0.47±1.07 before GnRHa treatment, 0.72±1.03 after 1 year treatment, and 0.72±0.98 after 2 years of GnRHa treatment; No significant changes were observed regarding the BMI SDS (P>0.05, P>0.05) (Table 2).
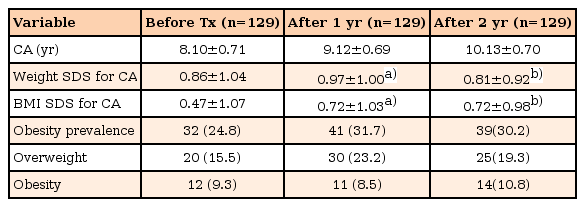
Changes in the weight SDS and BMI SDS following GnRHa treatment in girls with idiopathic central precocious puberty or early puberty
Before GnRHa treatment, 24.8% of the patients were overweight/obese, 31.7% were overweight/obese after 1 year of treatment, and 30.2% were overweight/obese after 2 years GnRHa treatment. A further subdivision of the 129 patients showed that before treatment, 20 patients (15.5%) were overweight, and 12 patients (9.3%) were obese. After 1 year of GnRHa treatment, 30 patients (23.2%) were overweight and 11 patients (8.5%) were obese. After 2 years of GnRHa treatment, 25 patients (19.3%) were overweight, and 14 patients (10.8%) were obese (Table 2). There were no significant changes with respect to the proportions of overweight/obesity patients after GnRHa treatment (P>0.05).
3. Weight SDS and BMI SDS changes in the different weight groups after GnRHa treatment
In the normal weight group, the weight SDS was 0.48±0.79 before treatment, 0.63±0.77 after 1 year of treatment, and 0.51±0.77 after 2 years of GnRHa treatment, and the changes in the weight SDS after 1 year and 2 years of treatment were not significant. In the overweight group, the weight SDS was 1.59±0.60 before treatment, 1.67±0.67 after 1 year treatment, and 1.48±0.61 after 2 years of GnRHa treatment were not significant. In the obese group, the weight SDS was 2.71±0.65 before treatment, 2.59±0.89 after 1 year treatment, and 2.17±0.68 after 2 years of treatment, and the changes in the weight SDS after 1 year and 2 years of treatment were not significant.
In the normal weight group, the BMI SDS increased significantly from 0.00±0.71 before treatment to 0.31±0.76 after 1 year of GnRHa treatment (P<0.0001). After 2 years of GnRHa treatment, the BMI SDS had increased significantly to 0.34±0.72 (P<0.0001) in the normal weight group. In the overweight group, the BMI SDS was 1.49±0.32 before treatment, 1.67±0.45 after 1 year of GnRHa treatment, and 1.70±0.58 after 2 years of treatment and the changes in the BMI SDS after 1 year and 2 years of treatment were not significant. In the obese group, the BMI SDS was 2.57±0.33 before treatment, 2.44±0.74 after 1 year of treatment, and 2.28±0.70 after 2 years of GnRHa treatment, and the changes in the BMI SDS after 1 year and 2 years of GnRHa treatment were not significant (Table 3).

Changes in the weight SDS and BMI SDS in girls with idiopathic central precocious puberty or early puberty following GnRHa treatment in 3 different BMI groups
4. Multiple regression analysis of the variables that influence the change of BMI SDS
A multiple regression analysis of the variables that may influence the change of BMI SDS (BMI SDS of after 2 years of GnRHa treatment – BMI SDS of before GnRHa treatment) revealed initial BMI SDS was the significant independent factor. Chronologic age and bone age at diagnosis, initial height SDS, initial body weight SDS and peak LH were not significantly affect the change of BMI SDS (Table 4).

Multiple regression analysis of the factors affecting the change of BMI SDS in girls with idiopathic central precocious puberty or early puberty
Discussion
In this study, GnRHa treatment did not significantly influence the BMI SDS in girls with CPP or EP as a whole group, even after 2 years of GnRHa treatment. However, the normal weight patients group showed a significant increase in the BMI SDS-CA after 2 years of GnRHa treatment.
An analysis of these results based on the degree of obesity, which involved dividing the patients into normal weight, overweight, and obese groups showed that the patients' weights increased significantly in all of the groups. However, regardless of the degree of obesity, the weight SDS change was not statistically significant. Hence, the weight gain that follows GnRHa treatment is not caused by the treatment itself, but it is associated with natural aging-related phenomena.
Within the study population of 129 patients, the proportion of overweight/obese patients changed from 24.8% before GnRHa treatment, to 31.7% after 1 year of treatment, and 30.2% after 2 years of treatment, but these changes were not significant. Before treatment, the normal weight group comprised 75.2% of the total population, which is consistent with a report that was published in 2005 year21), that stated that 19.0% of the total female population in Korea was overweight, and 9.7% was obese.
Puberty is occurring at increasingly younger ages worldwide, and the findings from one study has demonstrated similar trend in Korea22). Although genetic factors are considered one of the most important contributors to EP, other factors, including the nutritional status, obesity, and environmental factors, are also directly and indirectly related to EP23). In addition, obese children start developing breasts and pubic hair significantly earlier than children within normal weight ranges2425).
The proportions of overweight and obese patients among CPP patients were 48% and 26%, respectively, according to Palmert et al.13), 9.8% and 22.0%, respectively, according to GŁab et al.12), and 38.5% and 20.2%, respectively, according to Shiasi Arani and Heidari26), and 23.8% of CPP patients were (either overweight or obese) according to Arrigo et al.15). The proportions reported from these studies were higher than those determined in our study in which 15.5% and 9.3% of the patients were overweight and obese, respectively. While most researchers have reported that the proportions of overweight and obese populations did not change during their studies' follow-up periods with or without GnRHa treatment. Arrigo et al.15) reported reductions in the proportions of overweight and obese populations during their study's 44-month follow-up period. Ko et al.27) reported that GnRHa treatment did not increase the proportion of obese population in CPP patients. In this study, the proportions of overweight/obese patients were 24.8% (32 patients) before treatment, 31.7% (41 patients) after 1 year of treatment, and 30.2% (39 patients) after 2 years of treatment, hence, the proportions did not change significantly after treatment.
The results from studies of the influence of GnRHa treatment on the BMI have been inconsistent. In a study involving 110 CPP patients, the weight and BMI increased significantly in both the control and the GnRHa-treated groups after 1 year of treatment; however, there were no significant differences between the groups in relation to their BMI SDSs. Moreover, although the BMI SDS increased significantly in the GnRHa-treated group after 6 months of treatment, this increase was no longer apparent after 1 year of treatment. In addition, regardless of GnRHa treatment, the prevalence of obesity (overweight and obese) after 1 year was similar in the control and the GnRHa-treated groups26).
Similarly, the BMIs of the young patients in this study increased significantly from 17.47±2.21 kg/m2 before treatment, to 18.69±2.37 kg/m2 after 1 year of treatment, and to 19.47±2.47 kg/m2 after 2 years of treatment. On the contrary, the BMI percentile based on the chronological age remained on the same growth curve before and after treatment. While the BMI SDS also increased from 0.47±1.07 before treatment, to 0.72±1.03 after 1 year of treatment and 0.73±0.98 after 2 years of treatment, these changes were not statistically significant (P>0.05, P>0.05). These findings show that the BMI increases naturally as the length of the treatment period increases. Moreover, the lack of a significant increase in the BMI SDS signifies that GnRHa treatment is not associated with an increase in the BMI, a finding that is consistent with those from other studies1213).
However, in our analyses of the BMI and the BMI SDS-CA, in which the patients were divided into 3 groups based on their weights, both the BMI and the BMI SDS-CA showed statistically significant increases after 2 years of GnRHa treatment in the normal weight group. In the overweight group, the BMI increased significantly after 2 years of GnRHa treatment, but no significant changes were observed with respect to the BMI SDS-CA, regardless of the duration of treatment (1 year, P>0.05; 2 years, P>0.05). In the obese group, neither the BMI nor the BMI SDS-CA changed significantly, regardless of the duration of treatment. It is unclear why the BMI SDS-CA increased more remarkedly in the normal weight group compared with the other groups in this study.
Wolters et al.28) also reported that the influence of GnRHa treatment on weight and BMI increases varies depending on the degree of obesity. When the GnRHa treatment began, the BMI SDS increased consistently in the normal weight group, but it remained the same in the overweight group. Our study shows, in multiple linear regression analysis, a strong correlation between the change of BMI SDS and initial BMI SDS.
While the patients underwent short-term GnRHa treatments in most of the previously reported studies, Arrigo et al.15) reported BMI reductions in a study that involved long-term GnRHa treatment. In a study that involved long-term observations, Lazar et al.29) monitored 142 patients who had been diagnosed with CPP, and they reported that the mean BMI percentile was higher in the GnRHa-treated group than in the control group. However, the BMIs gradually decreased in all of the patients, regardless of whether or not they had received GnRHa treatment, and during the later stages of puberty, the BMI percentiles of patients who received the treatment and those who did not were not very different from one another.
Pasquino et al.30) studied 87 CPP patients, and their results showed that while the BMI increased consistently during the GnRHa treatment period, the BMI SDS-CA did not change significantly regardless of the length of the treatment period. Colmenares et al.31) reported a study that involved CPP and EP patients, and their results showed that the BMI z-scores and the proportions of the obese/overweight individuals did not change significantly with or without GnRHa treatment during the 3-year study period. When the GnRHa treatment ceased, the BMI z-scores declined in all of the patients. Therefore, the influence of GnRHa treatment on both the BMI and the BMI SDS decreased markedly in CPP and EP patients as the GnRHa treatment period lengthens, however, to confirm this, investigations into the changes in the BMI and BMI SDS after long-term GnRHa treatment are necessary.
Our study has some limitations that are described next. This was a cross-sectional retrospective study that involved a small sample size and a relatively short duration of treatment. Therefore, additional studies involving more patients, longer GnRHa treatment periods, and control groups are required to confirm the influence of GnRHa treatment in patients with CPP or EP.
In conclusion, BMI SDS increased in the GnRHa-treated patients as a whole group, but was not statistically significant. But BMI SDS increased significantly in the normal weight group after 2 years of GnRHa treatment. So, GnRHa treatment may affect the change of BMI SDS depending on degree of obesity.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.