Response to growth hormone according to provocation test results in idiopathic short stature and idiopathic growth hormone deficiency
Article information

Abstract
Purpose
To investigate growth response in children with either idiopathic short stature (ISS) or growth hormone (GH) deficiency (GHD).
Methods
The data of prepubertal GHD or ISS children treated using recombinant human GH were obtained from the LG Growth Study database. GHD children were further divided into partial and complete GHD groups. Growth response and factors predicting growth response after 1 and 2 years of GH treatment were investigated.
Results
This study included 692 children (98 with ISS, 443 partial GHD, and 151 complete GHD). After 1 year, changes in height standard deviation score (ΔHt-SDS) were 0.78, 0.83, and 0.96 in ISS, partial GHD, and complete GHD, respectively. Height velocity (HV) was 8.72, 9.04, and 9.52 cm/yr in ISS, partial GHD, and complete GHD, respectively. ΔHt-SDS and HV did not differ among the 3 groups. Higher initial body mass index standard deviation score (BMI-SDS) and midparental height standard deviation score (MPH-SDS) were predictors for better growth response after 1 year in ISS and the partial GHD group, respectively. In the complete GHD group, higher Ht-SDS and BMI-SDS predicted better growth response after 1 year. After 2 years of GH treatment, higher BMI-SDS and MPH-SDS predicted a better growth outcome in the partial GHD group, and higher MPH-SDS was a predictor of good growth response in complete GHD.
Conclusions
Clinical characteristics and growth response did not differ among groups. Predictors of growth response differed among the 3 groups, and even in the same group, a higher GH dose would be required when poor response is predicted.
Highlights
·Growth response did not differ among ISS, partial GHD, and complete GHD group.
·Predictors of growth response differed among groups.
·Predictors of good growth response were higher BMI-SDS and higher MPH-SDS in partial GHD; higher MPH-SDS in complete GHD.
Introduction
Growth hormone (GH) treatment is widely used to improve growth outcomes in children. However, to optimize GH treatment, researchers must investigate the treatment response and its predictive factors. Treatment response to GH is most commonly evaluated using height velocity (HV) or a gain in the height standard deviation score (Ht-SDS). Several criteria for poor first-year growth response have been proposed, such as a gain in Ht-SDS < 0.3 or < 0.5, a first-year HV < + 0.5 SD or < +1.0 SD for age and gender, or an increase in HV < 3 cm/yr [1]. According to a study that used the Pfizer International Growth Database, the following parameters were predictors of adult height in children receiving GH treatment: number of GH injections per week, duration of GH treatment, and birth weight. Midparental height (MPH)-SDS and Ht-SDS predicted growth response among children with GHD as well as among those with ISS [2]. In another study using the LG Growth Study database, age and MPH-SDS minus baseline Ht-SDS and BMISDS were predictive factors of first-year growth in patients with GHD [3].
In previous studies, children with ISS showed poorer long-term growth response than those with GHD after GH treatment. In the study of Hou et al. [4], HV after recombinant human GH (rhGH) therapy of 0.5 to 3 years was higher in the GHD group compared with the ISS group. Similar with this, in the study of Al Shaikh et al. [5], increase in Ht-SDS was higher in GHD compared to ISS at the end of the first year of rhGH therapy and after an average of 3 years. Thus, children with partial GHD are likely to have an intermediate growth response that falls between those of children with ISS and complete GHD. However, few studies have compared the growth response in partial GHD with that in complete GHD and ISS.
In the present study, we aimed to investigate growth response after 1 and 2 years of GH treatment in children with ISS, partial GHD, or complete GHD. We also attempted to compare growth response and predictive factors of growth response among these 3 groups.
Materials and methods
1. Subjects
Using the LGS Database, we obtained the data of prepubertal children with GHD or ISS who were treated using recombinant human GH (Eutropin Inj., Eutropin AQ Inj., LG Chem, Seoul, Korea). The LGS Database is an open-label, multicenter, prospective, and retrospective registry study started in 2012 to evaluate the long-term safety and effectiveness of 4 rhGH products [6,7].
The participants were patients with ISS and GHD treated using GH. Idiopathic GHD was defined using the following criteria: (1) height below the third percentile; (2) peak GH level below 10 µg/L in 2 standard stimulation tests; and (3) delayed bone age (BA) compared with chronological age (CA). The children with GHD were further divided into "complete GHD" (maximum GH peak < 5 µg/L) and "partial GHD" (maximum GH peak, 5–10 µg/L) groups. Patients with organic GHD were excluded because the treatment response can be greatly affected by underlying disease. ISS was diagnosed when a child had a current height below the third percentile for age but had normal GH responses in stimulation tests, normal birth weight, and no chromosomal abnormality.
In the LGS safety analysis set, there were 363 ISS and 1,412 GHD patients. Those who did not match the criteria of ISS or GHD were excluded. Those who did not have baseline height data, who were aged <2 years or >10 years when starting GH treatment, and those in the pubertal stage were also excluded. Ultimately, 692 subjects were included in the present study: 98 with ISS, 443 with partial GHD, and 151 with complete GHD.
2. Methods
Height, weight, body mass index (BMI), pubertal status, BA, insulin-like growth factor 1 (IGF-1), and IGF-binding protein-3 (IGFBP-3) values were recorded at baseline and at regular follow-ups conducted at 3- to 6-month intervals. We also obtained parental height and calculated midparental height (MPH). All SDS values of anthropometric measurements and IGF-1 were calculated using the Korean growth standard [8,9]. BA was determined using the Greulich and Pyle method [10].
We assessed the response to GH treatment by calculating changes in Ht-SDS (∆Ht-SDS) and HV for 1 and 2 years. We also analyzed the responses after dividing the subjects into 3 groups (ISS, partial GHD, and complete GHD).
3. Statistical analysis
All data are presented as mean±standard deviation. Differences in anthropometric measurements and treatment response were compared using analysis of variance and Kruskal-Wallis Test. Multivariate regression analysis was performed to evaluate the predictors of growth response. Variance inflation factors were controlled to <10 to avoid multicollinearity. All statistical analyses were performed using SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA), and P-values of <0.05 were considered statistically significant.
Results
1. Clinical characteristics of subjects
Clinical characteristics of patients are described in Table 1. Of the 692 subjects, 417 (60.3%) were male. The age at baseline was 6.0 years (range, 2–10 years). The Ht-SDS and BMI-SDS were -2.78±0.73 and -0.40±1.13, respectively. The IGF-1 SDS and IGFBP-3 SDS values were -0.72±0.93 and -0.44±2.69, respectively.
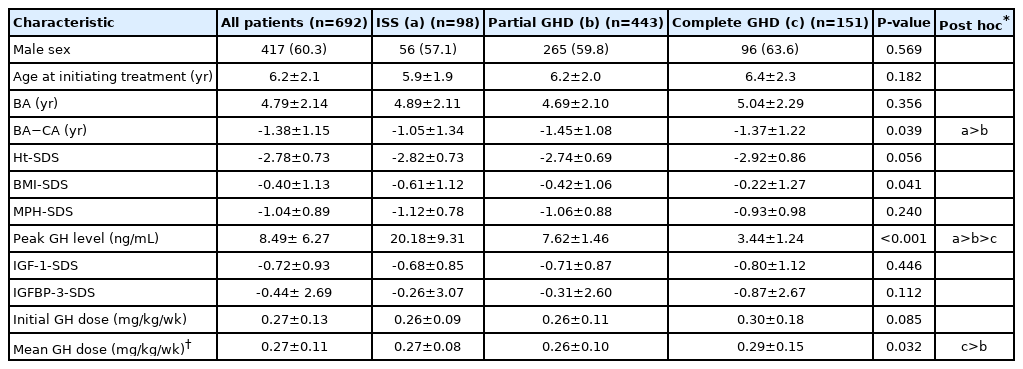
Clinical characteristics of participants
When compared, the 3 groups showed less delayed BA in the ISS group than the complete GHD group (BA–CA: -1.0 5±1.34 vs. -1.45±1.08, P=0.039). BMI-SDS was lower in the ISS group than in the complete GHD group (-0.61±1.12 vs. -0.22±1.27, P=0.041). Mean GH dose during the 2 years was higher in the complete GHD group than in the partial GHD group (0.29±0.15 mg/kg/wk vs. 0.26±0.10 mg/kg/wk, P=0.032). No differences were found in initial GH dose, initial age, initial BA, Ht-SDS, MPH-SDS, or IGF-SDS among the groups.
2. Growth response
HVs after 1 year of GH treatment were 8.72±1.64, 9.04±1.55, and 9.52±1.93 cm/yr in ISS, partial GHD, and complete GHD groups, respectively. ΔHt-SDS after 1 year of GH treatment was 0.78±0.40, 0.83±0.34, and 0.96±0.51 in ISS, partial GHD, and complete GHD groups, respectively. HV, ∆Ht-SDS, ∆BMI-SDS, and ∆(BA–CA) after 1 year and 2 years of GH treatment did not differ among the groups. But, ∆Ht-SDS during the second year of treatment showed a difference among the groups (ISS < partial GHD < complete GHD: 0.29 vs. 0.39 vs. 0.53, P=0.032) (Table 2).

Growth response after growth hormone treatment
3. Predictors of growth response
1) After 1 year
We performed univariate analysis with 9 possible predictors (age at start of GH treatment, sex, BA, initial Ht-SDS, initial BMI-SDS, MPH-SDS, IGF-1-SDS, peak GH level, and initial GH dose). We then performed a multivariate regression analysis with factors extracted based on univariate analysis.
In ISS patients, BMI-SDS was a positive predictor of ΔHt-SDS and HV. Higher MPH-SDS predicted better growth outcome in the partial GHD group. In the complete GHD group, initial Ht-SDS and BMI-SDS were positive predictors of good growth outcome (Table 3, Fig. 1).

Results of multivariate regression analysis of factors associated with growth response during 1 year of GH treatment
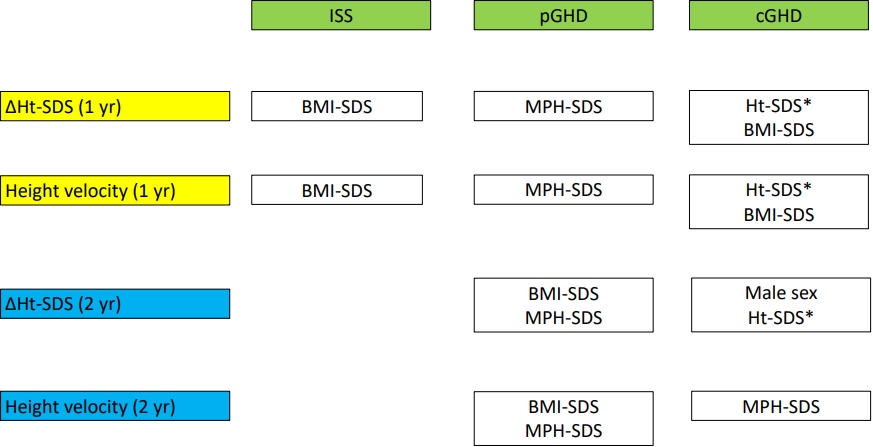
Predictors of growth response. ISS, idiopathic short stature; GHD, growth hormone deficiency; Ht, height; pGHD, partial GHD; cGHD, complete GHD; SDS, standard deviation score; BMI, body mass index; MPH, midparental height. *Ht-SDS is a negative predictor, and all the others are positive predictors.
2) After 2 years
We also investigated predictors of GH response after 2 years in partial and complete GHD groups. Higher BMI-SDS and MPH-SDS predicted better growth outcome in the partial GHD group. In the complete GHD group, higher Ht-SDS predicted higher ΔHt-SDS, and MPH-SDS was a positive predictor of HV (Table 4, Fig. 1).
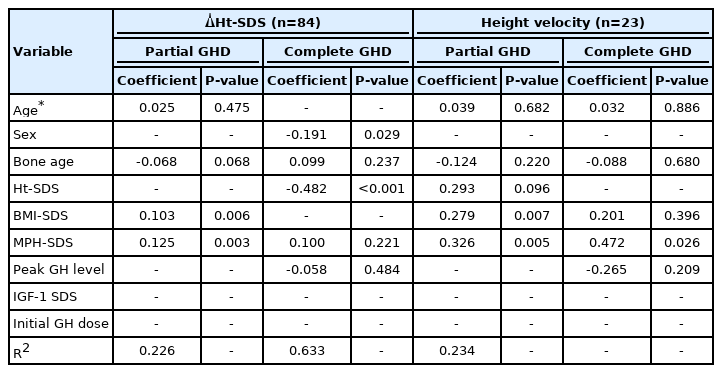
Results of multivariate regression analysis of factors associated with growth response during 2 years of GH treatment
Discussion
This study investigated the growth response to GH therapy in 3 groups (ISS, partial GHD, and complete GHD). The baseline clinical features and growth outcome did not differ, but predictors of growth response differed among the groups.
GHD is diagnosed by the maximum peak GH level. However, GHD diagnosis remains difficult because of the wide variation observed in normally growing children [11]. More than 20% of children with normal stature show GH peak level <10 ng/mL [12], so GHD, especially partial GHD, can be overdiagnosed. Many external factors, such as fasting, physical activity, heat exposure, and sleep, can also influence the GH stimulation test [13]. The GHD group had clinical features similar to those of the ISS group, perhaps because we used a high cutoff value of GH peak level. There is no consensus cutoff value of GH to diagnose GHD. In some studies that used monoclonal antibody testing, a lower cutoff value of 6–7 ng/mL was suggested [14]. However, in this multicenter study, various testing methods were used, so we used a conventional cutoff value of 10 ng/mL [15,16]. This might have diminished the differences among the groups. Moreover, we could not assess the growth velocity or IGF-1 level before enrollment, which might have caused misclassification. Recently, the Korean growth curve has been revised, and the third percentile height to diagnose short stature has increased; thus, more children are being diagnosed with short stature or GHD, and careful patient selection for GH treatment will be more important.
When comparing growth response, ∆Ht-SDS and HV during 1 year did not differ among the groups. The results of previous studies have been controversial in this regard. Several studies have reported similar growth responses between the ISS and GHD groups [17-19]. However, Kim et al. [20] reported that ∆HtSDS in patients with idiopathic GHD was significantly higher than that in patients with ISS. We were particularly interested in the lack of difference in growth response between the partial and complete GHD groups. In this regard, several studies have investigated the difference in growth response to GH between partial and complete GHD and found conflicting results. Some have reported that the partial GHD group showed a lower growth response than the complete GHD group [18,21]. In contrast, Cardoso et al. [22] found no difference in growth response after 1 year of GH treatment between the complete and partial GHD groups.
Partial and complete GHD had different predictors of growth response. Ht-SDS and BMI-SDS were predictors of growth response in complete GHD. MPH-SDS was a predictor of growth response in the partial GHD group. Baseline Ht-SDS has been suggested as a predictor of growth response in the literature [21,23]. BMI-SDS was also suggested as positive predictor of GH response in GHD children [24]. This is thought to be related to relatively higher GH doses in obese children. MPH and BMI have been reported in previous studies as predictors of growth response in children with GHD [25-27]. A higher MPH compared with current height was a predictive factor of good growth response to GH in the ISS group in a previous study [28]. It might be that, in the partial GHD group, genetic growth potential is not significantly decreased, so growth response is related to MPH as in the ISS group.
The maximum peak GH level has been reported as a predictive factor of growth response in several studies, though it was not a significant predictive factor in our study. For instance, in a study by Cole et al. [29], the maximum peak GH level was a predictive factor of growth response in children with GHD. Bright et al. [30] also reported that treatment outcome was correlated with maximum peak GH level in a patient group with GHD or ISS.
Another important predictor of GH response is dosage. Because children with ISS might require supraphysiologic level of IGF-I to obtain the desired height gain, a higher dose is usually recommended in children with ISS than in children with GHD [31]. However, initial doses were not different among the groups in the present study. This is probably because the dose covered by national health insurance for GHD was used in most cases, even in the ISS group. Considering the poor treatment response in the ISS group, a higher initial dose and a more rapid GH dose escalation would be required, especially when poor response is predicted.
Male sex was a positive predictor of ΔHt-SDS after 2 years. Similar with our result, one previous study reported that ΔHSDS was significantly greater in boys than girls in prepubertal GHD children. In their study, difference in growth response is thought to be independent of changes in IGF-I level, which implicate factors other than IGF-I in the gender-related modification of growth response in young children [32].
Comparing predictors of 1-year growth response with those of 2 years, the partial GHD group had the same predictors. In the complete GHD group, the predictors were different; 1-year growth response was predicted by initial Ht-SDS and BMI-SDS, while 2-year growth response was predicted by MPH-SDS. One explanation is that growth response is determined by genetic potential after initial catch-up growth in the GHD group.
Our study had several limitations. First, the number of subjects in the ISS group was relatively small. Predictors of 2-year growth response could not be obtained for the ISS group due to the small number of patients. Second, we did not include compliance as a possible predictor, but it is an important factor affecting growth response. In the present study, most participants visited the hospital regularly; thus, adherence to GH treatment was probably higher in the study participants than in nonparticipants. Finally, we only evaluated the short-term growth response. Long-term follow-up data are necessary to obtain long-term growth response during GH treatment, as assessed by final height. Despite these limitations, our results provide meaningful data regarding growth response and the predictors of growth response in short children.
In conclusion, the current diagnosis of GHD and ISS in the clinical field might be insufficient to classify clinically distinct groups. Treatment response after 1 year did not differ among the groups, but ∆Ht-SDS during the second year of treatment was different among the groups (complete GHD>partial GHD>ISS). Each group has distinct or common predictors of growth outcome, and even in the same group, a higher dose would be required for patients with poor response is predicted.
Notes
Ethical statement
Informed consent was obtained from all the participants, and the Institutional Review Board (IRB) of Pusan National University Yangsan Hospital approved the study (IRB #05-2018-140)
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contribution
Conceptualization: JHY; Data curation: CKC; Formal analysis: JHL, JK, MJK; Methodology: HJK; Project administration: YJK; Visualization: JEL, WYC; Writing - original draft: JYY; Writing - review & editing: JHY
Acknowledgements
The authors thank all of the investigators of "LG Growth Study," who contributed their data, as well as LG Chem Ltd. for providing statistical analysis. We would like to thank eWorld Editing (eworldediting.com) for the English language editing.