Short-term efficacy of 1-month and 3-month gonadotropin-releasing hormone agonist depots in girls with central precocious puberty
Article information

Abstract
Purpose
Gonadotropin-releasing hormone agonist (GnRHa) has been the mainstay of central precocious puberty (CPP) treatment for decades, but few reports have compared the efficacy of 1-month and 3-month depot GnRHa formulations. This study investigates the short-term efficacy of 1-month and 3-month GnRHa depots in girls with CPP.
Methods
Overall, 150 girls with CPP were included in a retrospective review of medical records. Subjects in group 1 (n=105) were treated with 1-month GnRHa depots for ≥12 months, and those in group 2 (n=45) were treated with 1-month GnRHa depots for 6 months followed by 3-month GnRHa depots for ≥6 months. Anthropometric and biochemical data were compared between the groups at 3-time points (after 0, 6, and 12 months of GnRHa treatment).
Results
Demographic and clinical characteristics did not differ between the groups at baseline or after 6 months of GnRHa treatment. After 12 months of GnRHa treatment, patients in the both groups showed no difference in bone age (BA), chronological age (CA), BA–CA difference, height standard deviation score (SDS) for CA and BA, or body mass index SDS for CA and BA. The sexual maturity rate of the breast was prepubertal at 12 months in most of subjects. GnRH-stimulated luteinizing hormone (LH) level was suppressed during GnRHa treatment in both groups at 6 and 12 months, although the LH level in group 2 was higher than that in group 1.
Conclusions
Treating CPP with a 3-month GnRHa depot showed short-term efficacy comparable to that with a 1-month depot in anthropometric parameters and pubertal suppression.
Highlights
· In Korea, 1-, 3-, and 6-month depot formulations of GnRHa have been approved for treatment of CPP.
· Treatment with a 3-month GnRHa depot in CPP girls was comparable to that with a 1-month depot in many clinical aspects.
· A 3-month depot formulation of GnRHa could be a viable option for treatment of CPP.
Introduction
Central precocious puberty (CPP) in girls is defined as the onset of breast development before 8 years of age as a result of premature activation of the hypothalamic-pituitary-gonadal axis [1,2]. Early menarche can cause short adult stature because of early epiphyseal closure and emotional, behavior, and mood fluctuations because of physical differences from peers with normal puberty [2,3]. To prevent the adverse outcomes of CPP, early diagnosis and appropriate treatment are essential. After biochemical confirmation of CPP using gonadotropin-releasing hormone (GnRH) stimulation tests in patients with early signs of puberty, a depot formulation of a GnRH agonist (GnRHa) is used as standard therapy [4].
Because continuous GnRH secretion, rather than intermittent exposure to it, suppresses pubertal development by desensitizing and downregulating pituitary GnRH receptors, GnRHa is used to treat CPP [5]. Several previous studies have reported that GnRHa treatment in CPP regresses pubertal symptoms and signs and increases predicted adult height (PAH) [2,5-7]. In Korea, several doses of depot formulations of GnRHa, leuprolide (3.75 mg and 11.25 mg), and triptorelin (3.75 mg, 11.25 mg, and 22.5 mg) have been approved for treatment of CPP. The most commonly used GnRHa formulation is a 1-month depot.
Previous reports have demonstrated that treating CPP with a 3-month formulation can suppress pubertal development more efficiently than can a 1-month formulation [8-10]. Treatment with a 3-month preparation could reduce the burden of injections and improve convenience and compliance [11]. However, few reports have evaluated the effects of switching medication from the 1-month to the 3-month formulation [8]. Additionally, no clinical information is available about 3-month GnRHa treatment in Korean CPP patients. Therefore, this study compares the short-term efficacy in terms of anthropometric and laboratory parameters of a 3-month GnRHa depot with that of a 1-month depot in girls diagnosed with CPP.
Materials and methods
1. Subjects
Girls diagnosed with CPP at the Pediatric Endocrinology Clinic of Seoul National University Bundang Hospital from January 2016 to December 2018, were considered as potential candidates for this study. The inclusion criteria were as follows: (1) breast development before the age of 8 years, (2) advancement of bone age (BA) over chronological age (CA), (3) peak luteinizing hormone (LH) level ≥5 IU/L in the GnRH stimulation test, (4) start of GnRHa treatment at the age of 7.0–8.9 years, and (5) GnRHa treatment using a 1-month depot formulation for ≥12 months or a 1-month depot formulation for 6 months followed by a 3-month depot formulation for ≥6 months. Among the 264 subjects who met the inclusion criteria, 150 girls with CPP were included in this study after exclusion of subjects with (1) CPP caused by organic brain lesions such as brain tumors or anomalies (n=11); (2) endocrinological disorders such as hypothyroidism, hyperthyroidism, or adrenal disease (n=13); (3) chronic illness such as diabetes mellitus or inflammatory disorders (n=30); or (4) a history of recombinant human growth hormone treatment (n=60).
2. Methods
Data were obtained from a retrospective review of medical records. The following demographic and anthropometric data were collected before treatment and after 6 months and 12 months of GnRHa treatment: CA, BA, height, weight, body mass index (BMI), sexual maturity rating (SMR), midparental height, and birth weight. Height was measured using a Harpenden Stadiometer (Holtain Ltd., Crosswell, UK), and weight was measured using an electric balance (GL-310; G-Tech International Co. Ltd., Seoul, Korea). BMI was calculated as weight in kilograms divided by height in meters squared. Height and BMI were transformed into standard deviation score (SDS) for the corresponding CA and BA using the 2017 Korean National Growth Charts [12]. BA from plain radiographs of the left hand was interpreted by a single pediatric endocrinologist using the Greulich-Pyle method [13]. SMR was assessed using the Marshall and Tanner method [14]. PAH was calculated according to the Bayley-Pinneau method [15].
For diagnosis of CPP, all subjects underwent GnRH stimulation tests using an intravenous injection of 0.1 mg of synthetic GnRH (Relefact; Sanofi-Aventis, Frankfurt, Germany). Blood samples were obtained before and at 15, 30, 45, and 60 minutes after GnRH injection to measure LH, follicle-stimulating hormone (FSH), and estradiol. Basal and peak levels of LH and FSH and basal estradiol level were used for the analysis. LH and FSH levels were measured using immunoradiometric assays, and estradiol level was measured via radioimmunoassay (DIAsource, Ottignies-Louvain-la-Neuve, Belgium).
Study subjects were divided into 2 groups according to mode of GnRHa administration (Fig. 1). Group 1 (n=105) comprised subjects treated with a 1-month depot formulation of GnRHa (leuprolide acetate; Leuplin depot 3.75 mg, Takeda, Tokyo, Japan) every 4 weeks for at least 1 year. Group 2 (n=45) comprised subjects treated with a 1-month depot formulation of GnRHa (leuprolide acetate; Leuplin depot 3.75 mg, Takeda) every 4 weeks for the first 6 months of treatment and then with a 3-month depot formulation (leuprolide acetate; Leuplin DPS depot 11.25 mg, Takeda) administered every 3 months for at least 6 months. Initially, 60–90 μg/kg of leuprolide acetate was administered subcutaneously every 4 weeks for all subjects. In group 2, the dose of the 3-month depot formulation was 3 times the last dose of the 1-month depot formulation. The dose of each formulation was adjusted according to growth rate and SMR. Every 6 months, the LH level was measured 30 minutes after administration of synthetic GnRH. Stimulated LH level less than 3 IU/L indicated sufficient pubertal suppression [16].

Scheme of the present study.
3. Statistical analyses
Data analysis was performed using Stata 16.1 (StataCorp LP, C ollege Station, T X, USA). Data are presented as mean±standard deviation for continuous variables and as number and percentage of subjects for categorical variables. Student t-test and Fisher exact test were used to compare groups 1 and 2. For comparison of continuous or categorical variables obtained at 3-time points in each group, repeated measures analysis of variance or Fisher exact test was used, respectively. A P-value less than 0.05 was considered statistically significant.
Results
1. Baseline characteristics of the study subjects
The baseline characteristics of the 150 patients enrolled in this study are presented in Table 1. The mean CA and BA and the difference between BA and CA were 8.4±0.6 years, 10.0±0.7 years, and 1.6±0.7 years, respectively, which revealed no difference between groups (all P>0.05). Furthermore, there were no significant differences in height SDS for CA and BA, BMI SDS for CA and BA, or PAH. Although breast SMR was higher in group 2 than in group 1 (P<0.001), there was no difference between basal or peak LH and FSH levels or basal estradiol level between the 2 groups. The GnRHa dose in group 2 was significantly higher than that in group 1 (84.9±9.0 μg/kg/mo vs. 78.4±9.3 μg/kg/mo, P<0.001).

Baseline demographic and clinical characteristics of study subjects
2. Changes in clinical parameters during GnRHa treatment
During treatment, subjects in both groups showed significant decrease in BA–CA difference and height SDS for CA and significant increase in height SDS for BA, BMI SDS for CA and BA, and PAH (Table 2, Fig. 2). Breast SMR regressed significantly in both groups. Among the participants, 6.7% after 6 months and 4.7% after 12 months of GnRHa treatment showed a breast SMR of 2, but the difference between the groups was not significant. LH level after GnRH stimulation was suppressed at 6 months and sustained at 12 months in both groups (1.1±0.5 IU/L at 6 months and 1.1±0.4 IU/L at 12 months in group 1 and 1.2±1.0 IU/L at 6 months and 1.4±0.5 IU/L at 12 months in group 2). At 6 months, 2 patients in group 2 were not suppressed biochemically, but all patients showed LH level < 3 IU/L at 1 year.

Comparison of clinical parameters between groups at 6 and 12 months by groups after gonadotropin-releasing hormone (GnRH) agonist treatment
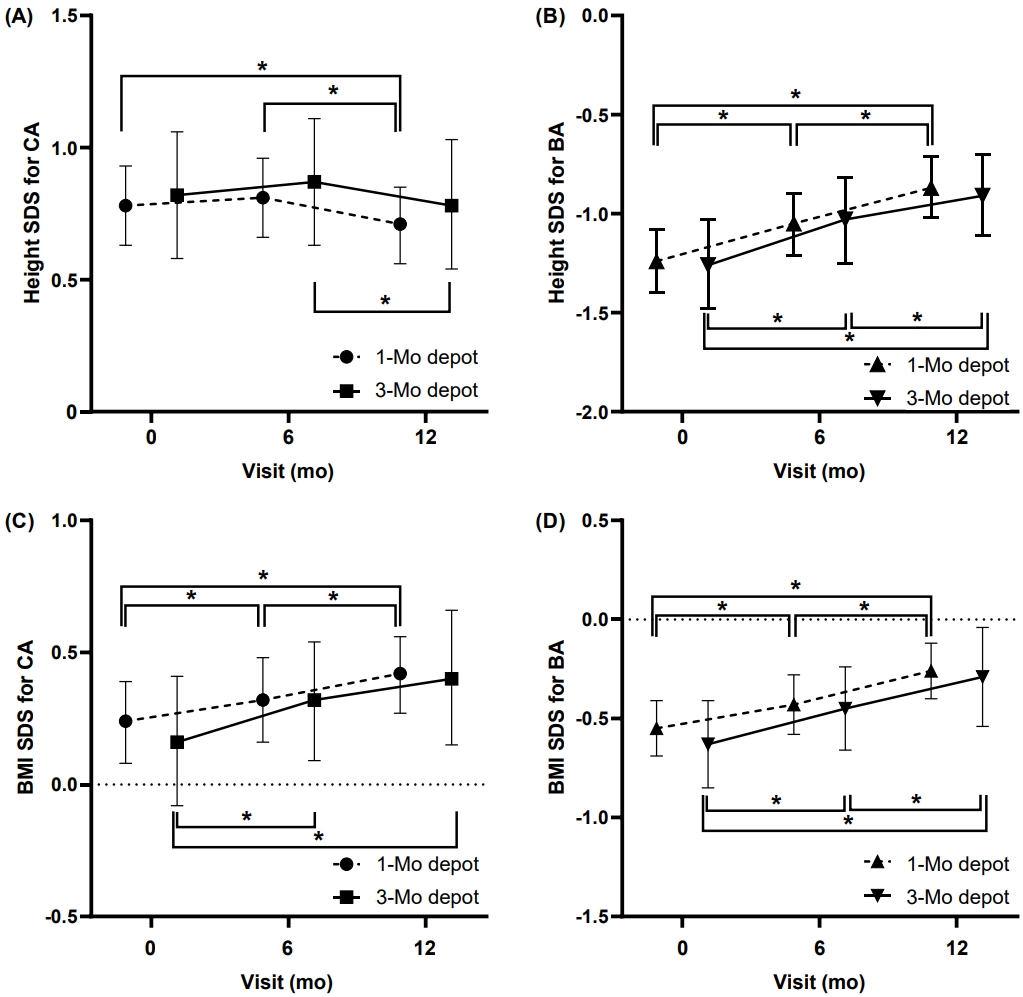
Changes in height SDS for CA (A), height SDS for BA (B), BMI SDS for CA (C), and BMI SDS for BA (D) by group and visit. SDS, standard deviation score; CA, chronological age; BA, bone age.
3. Comparison between groups at 6 months and 1 year of GnRHa treatment
After 6 and 12 months of GnRHa treatment, CA, BA, BA–CA difference, height SDS for BA and CA, BMI SDS for BA and CA, PAH, and PAH SDS did not differ significantly between groups (Table 2, Fig. 2). The LH level after GnRH stimulation in group 2 was significantly higher than that in group 1 (1.1±0.4 IU/L vs. 1.4±0.5 IU/L, P<0.001) after 12 months of treatment but was suppressed in all subjects. The dose of GnRHa (μg/kg/mo) did not differ significantly between the groups after 6 or 12 months of GnRHa treatment. In both groups, breast SMR was suppressed (Table 2).
Discussion
Long-acting GnRHas have been the standard treatment for CPP since the mid-1980s [2]. In this study, we compared the efficacy of a 3-month depot formulation of GnRHa with that of a 1-month depot in girls with CPP. During the 6-month period of comparison between the 1-month and 3-month GnRHa treatments, we found no differences in anthropometric, radiographic, or laboratory parameters between groups. This indicates that the 3-month depot GnRHa formulation has short-term efficacy comparable to that of the 1-month depot. Although the LH level after GnRH stimulation was higher in group 2 than in group 1 at 12 months, LH level was sufficiently suppressed in all subjects in both groups.
In CPP patients, GnRHa administration suppresses pubertal progression by desensitizing and downregulating pituitary GnRH receptors. In this study, breast SMR was decreased after 6 and 12 months of GnRHa treatment in both groups. Moreover, GnRH-stimulated LH level showed sufficient suppression of pubertal development with both GnRHa formulations. Other studies of a 3-month depot formulation reported similar results. Carel et al. [17] observed that a 3-month depot formulation of leuprolide acetate (11.25 mg) effectively suppressed gonadotropin secretion. A 36-month study showed that a 3-month depot of leuprolide acetate effectively suppressed pubertal symptoms and signs without causing any new adverse effects [18]. A triptorelin 11.25 mg 3-month depot also effectively suppressed LH level [19]. In that study, the GnRHa dose (μg/kg/mo) decreased during the treatment period because of weight gain (Table 2). In this study, the GnRHa dose (mg/mo) had not changed when pubertal signs were sufficiently suppressed.
Several studies have shown that GnRHa treatment improves the final height of CPP patients [7,20]. Fuld et al. [10] reported that administering GnRHa using a 1-month 7.5 mg, 3-month 11.25 mg, or 3-month 22.5 mg formulation showed effective suppression without causing any significant difference in height, BA, or PAH among groups. Bertelloni et al. [21] showed similar adult heights between girls treated with monthly (3.75 mg) or quarterly triptorelin (11.25 mg). Our results are consistent with those of previous studies. The height SDS for BA and PAH increased during treatment in both groups. Furthermore, the BA–CA difference decreased during treatment, indicating an attenuation of BA advancement with both GnRHa depots. Some studies showed that greater LH suppression increased PAH [22,23]. In this study, after 12 months of treatment, the LH level was higher in the 3-month depot group than in the 1-month depot group, but PAH showed no significant difference (160.2±5.8 cm for group 1 and 159.8±5.0 cm for group 2). Further long-term studies with leuprolide acetate are required to assess the final height.
There has been controversy about the association between GnRHa treatment and weight gain or obesity [24]. Several studies have shown increased BMI SDS during GnRHa treatment and decreased BMI SDS after discontinuation of GnRHa [25-28]. In a study with a 1-month GnRHa depot formulation, the proportion of normal weight, overweight, and obese subjects did not differ significantly before and after discontinuation of GnRHa treatment [28]. An increase in BMI SDS during GnRHa treatment might reflect relatively more weight gain than height gain because of pubertal suppression by GnRHa. In this study, GnRHa treatment significantly increased BMI and BMI SDS in both groups during 1 year of GnRHa treatment, which is in concordance with previous studies [26,28]. However, the type of GnRHa made no significant difference in the BMI SDS change. Additional long-term follow-up is required.
The doses of GnRHa administered to treat CPP vary worldwide. In the United States, the recommended starting doses for 1-month and 3-month depot leuprolide preparations range from 7.5 mg to 15 mg and 11.25 mg to 30 mg, respectively [29]. On the contrary, Europe and Asia have established a lower standard dose of 3.75 mg [30,31]. Although the dose of GnRHa in CPP patients in Korea and Asia is lower than that in other countries, low-dose GnRHa treatment efficiently suppressed the pituitarygonadal axis, and PAH was not different from those treated with a higher dose [32,33]. After 12 months of GnRHa treatment in both groups, pubertal symptoms had regressed and stabilized, and LH level was suppressed.
Our study has several limitations. First, this was a retrospective, single-center study with a relatively short duration. Second, we did not evaluate adverse events with either the 1-month or 3-month depot. However, all subjects in both groups tolerated each GnRHa formulation well and continued to use it for at least 12 months. Despite its limitations, this study is the first to compare the efficacy of 1-month and 3-month depot formulations of GnRHa in Korean patients with CPP.
In conclusion, the 3-month depot formulation of GnRHa effectively suppressed the pituitar y-gonadal axis and gonadotropin secretion in girls with CPP. Treatment with a 3-month GnRHa depot was comparable to that with a 1-month depot in terms of successful inhibition of pubertal progression, attenuation of BA advancement, and increased PAH after a safe switch from the monthly formulation. Because it offers improved convenience and compliance, a 3-month depot formulation could be a viable option for treatment of CPP. Further long-term prospective studies are required to confirm our results and investigate treatment safety.
Notes
Ethical statement
This study was approved by the Seoul National University Bundang Hospital Institutional Review Board (IRB) (IRB number: B-2005-613-113), and the requirement for informed consent was waived by the IRB.
Conflicts of interest
JHK received an honorarium from Takeda, Ferring, and Ipsen. No other potential conflicts of interest relevant to this article are reported.