Association of metformin and statin medications with surrogate measures of cardiovascular disease in youth with type 1 diabetes: the SEARCH for diabetes in youth study
Article information

Abstract
Purpose
Youth with type 1 diabetes mellitus (T1DM) are at risk of cardiovascular disease (CVD). We evaluated if metformin or statin use was associated with surrogate measures of improved CVD.
Methods
We included participants from the SEARCH observational study. Participants treated with insulin plus metformin (n=42) or insulin plus statin (n=39) were matched with 84 and 78 participants, respectively, treated with insulin alone. Measures of arterial stiffness obtained were pulse wave velocity (PWV), augmentation index (AI75), and heart rate variability as standard deviation of the normal-to-normal interval (SDNN) and root mean square differences of successive NN intervals (RMSSD).
Results
CVD measures were not significantly different among participants on insulin plus metformin versus those on insulin alone: PWV (5.9±1.0 m/sec vs. 5.8±1.5 m/sec, P=0.730), AI75 (1.8 [-6.0 to 8.0] vs. -2.4 [-10.7 to 3.8], P=0.157), SDNN (52.4 [36.8–71.1] m/sec vs. 51.8 [40.1–74.9] m/sec, P=0.592), and RMSSD (43.2 [29.4–67.6] vs. 47.4 [28.0–76.3], P=0.952). CVD measures were not different for statin users versus nonusers: PWV (5.7±0.8 m/sec vs. 5.9 ±1.1 m/sec, P=0.184), AI75 ( -4.0 [-9.5 to 1.7] vs. -6.7 [-11.3 to 5.7], P=0.998), SDNN (54.6 [43.5–77.2] m/sec vs. 63.1 [44.2–86.6] m/sec, P=0.369), and RMSSD (49.5 [31.2–74.8] vs. 59.2 [38.3–86.3], P=0.430).
Conclusions
We found no associations of statin or metformin use with surrogate measures of CVD. Future prospective pediatric clinical trials could address this issue.
Introduction
Youth with type 1 diabetes mellitus (T1DM) have an increased lifetime risk for cardiovascular disease (CVD) [1]. Low insulin sensitivity (IS) and dyslipidemia, among others, have been implicated in this increased risk [1].
Low IS contributes to higher CVD risk in both youth and adults with T1DM [2-4]. Our group previously found that youth with T1DM and low IS also have higher arterial stiffness as assessed by pulse wave velocity (PWV), a surrogate measure of CVD [5]. Data from the Pittsburgh Epidemiology of Diabetes prospective study of 602 adults with T1DM showed that those with low versus normal IS had a higher 10-year incidence of nonfatal myocardial infarct and mortality [2]. Furthermore, women with T1DM and low IS lose the known cardioprotection of female sex [3]. Similar to adult studies, nonobese adolescents with T1DM and lower IS have a more atherogenic lipoprotein profile, i.e., lower low-density lipoprotein cholesterol (LDL-C) than healthy controls, and this atherogenic distribution correlates with low IS [6]. In addition, lean adolescents with T1DM and low IS have impaired functional exercise capacity and evidence of diastolic dysfunction and left ventricular hypertrophy [4].
Dyslipidemia is an established risk factor for CVD in individuals with and without diabetes [1]. Previous studies, including those from our group, found that dyslipidemia in youth with T1DM is associated with increased carotid intima media thickness (CIMT) and higher arterial stiffness, measured as increased PWV [7,8].
Arterial stiffness is widely used as a surrogate marker of CVD, and studies in adults show a association of increased arterial stiffness with future CVD events [9]. For 1,746 youth with T1DM in the SEARCH cohort study, we reported an 11.6% age-adjusted prevalence of increased arterial stiffness [10]. Our group and others found higher arterial stiffness in youth with T1DM compared to healthy controls [11-14]. Furthermore, our group previously found an association of increased arterial stiffness with low IS in youth with T1DM [11]. Another surrogate marker for subclinical CVD is heart rate variability (HRV). Decreased HRV is a sign of diabetic neuropathy and indicates the presence of cardiac autonomic dysfunction. Decreased HRV is associated with a 32%–45% increased risk of CVD events in individuals without previously established CVD [15-18]. In the SEARCH cohort study, we reported a 14.4% age-adjusted prevalence of cardiovascular autonomic neuropathy [10]. We also showed that youth with T1DM had decreased HRV, which is associated with increased arterial stiffness and poor glycemic control [15,19,20].
Medications that improve IS and dyslipidemia improve CVD in adults with type 2 diabetes mellitus (T2DM), but use of these medications to manage youth with T1DM is still controversial [1,21]. Metformin is a first-line agent for T2DM but is often used "off label" by pediatric endocrinologists, especially in youth with obesity and T1DM. Most studies found that metformin had no benefit for improving glycemic control in T1DM but reduced total daily insulin dose requirements and body mass index (BMI) in youth with obesity and T1DM [22]. Statins, which are medications to improve total and LDL-C, reduce cardiovascular events in adults with diabetes, but few studies have investigated the effect of statins on surrogate measures of CVD in youth with T1DM [23,24].
Our objective was to evaluate if treatment with metformin or statins was associated with decreased CVD risk as assessed by arterial stiffness, using data from the SEARCH for Diabetes in Youth study.
Materials and methods
1. Participants
The SEARCH for Diabetes in Youth study was initiated in 2000 in five sites across the United States to improve understanding about youth-onset diabetes and its complications. Individuals diagnosed with diabetes before age 20 were identified from a population-based incidence registry network at five U.S. sites (South Carolina; Cincinnati, Ohio and surrounding counties; Colorado with southwestern Native American sites; Seattle, Washington, and surrounding counties; and Kaiser Permanente Southern California members from 7 counties) by the SEARCH for Diabetes in Youth Registry Study [10]. Patients newly diagnosed with T1DM in 2002-2006 or 2008 were identified from ongoing surveillance of networks of hospitals and health care providers.
Patients who could be contacted were recruited for a baseline visit at a mean and standard deviation (SD) of 9.3±6.4 months from diagnosis. A subset of participants with at least 5 years diabetes duration (to increase the likelihood of detecting complications) who were aged 10 years or older were recruited for a follow-up visit between 2012–2015, a mean (SD) of 7.9±1.9 years from diagnosis [10]. A flowchart of the SEARCH cohort study has been published [10].
2. Data collection
At both baseline and follow-up visits, trained personnel administered questionnaires to participants obtained fasting blood samples, and performed anthropometric measurements as previously described [10]. Race/ethnicity was self-reported and categorized into non-Hispanic white and minority racial/ethnic groups, including Hispanic (regardless of race), non-Hispanic black, American Indian, Asian/Pacific Islander, and other or multiple races/ethnicities. BMI was calculated as weight in kilograms divided by height in meters squared and converted to a z-score. Three systolic and diastolic blood pressure levels were obtained after at least 5 minutes of rest and averaged for inclusion in the analysis.
At both visits, a fasting blood draw occurred after an 8-hour overnight fast, and medications such as short-acting insulin were withheld the morning of the research visit. Samples were processed locally and shipped to a central laboratory (Northwest Lipid Metabolism and Diabetes Research Laboratories, University of Washington, Seattle, WA, USA), where high-density lipoprotein cholesterol (HDL-C), LDL-C, triglycerides (TG), and glycosylated hemoglobin (HbA1c) were measured. HbA1c was measured with high-performance liquid chromatography (TOSOH Bioscience, Inc., San Francisco, CA, USA). TG and HDL-C were measured using Roche Modular P (Roche Molecular Biochemical Diagnostics, Indianapolis, IN, USA). LDL-C was calculated by the Friedewald equation for participants with triglyceride concentration <400 mg/dL and by the beta quantification procedure for those with TG≥400 mg/dL, as previously described [11]. IS score was calculated based on a previously described equation developed and validated among SEARCH participants using data from a euglycemic–hyperinsulinemic clamp [25]: log IS=4.64725−0.02032 (waist, cm)−0.09779 (HbA1c, %)−0.00235 (TG, mg/dL). Lower IS score indicated lower IS.
At the follow-up visit, arterial stiffness and HRV measurements were performed using a SphygmoCor Cardiovascular System (AtCor Medical, Naperville, IL, USA) as previously described [11,15]. Higher carotid-femoral PWV and higher augmentation index (AI75) indicated higher arterial stiffness and were used as surrogate markers of CVD. Three measurements of PWV and three measurements of AI75 were performed after the participant rested for 10 minutes. Results were averaged. Time domain indices of HRV used in analyses were standard deviation of the normal-to-normal interval (SDNN) and root mean square differences of successive NN intervals (RMSSD). Reduced SDNN indicated reduced overall HRV, and reduced RMSSD indicated loss of heart parasympathetic tone activity. Data associated with dose, duration of therapy, and compliance of metformin and statin use were not available.
3. Study design and statistical analysis
To evaluate the effects of metformin on surrogate measures of CVD, we selected all SEARCH participants with T1DM who reported taking insulin and metformin at the follow-up visit (n= 42, group 1). A propensity score was used to individually match group 1 participants on a 1:2 ratio to youth with T1DM who, at the follow-up visit, were treated with insulin only (n=84, reference group 1). The propensity score was developed using age, sex, race, IS score, non-HDL-C, BMI z-score, HbA1c, and systolic blood pressure (SBP) z-score measured at the baseline visit (Table 1). A similar process was used to evaluate the effects of statins on surrogate measures of CVD using data from SEARCH participants with T1DM who reported taking insulin and a statin at the follow-up visit (n=39, group 2). Group 2 participants were individually matched on a 1:2 ratio to youth with T1DM who, at the follow-up visit, were treated with insulin only (n=78, reference group 2). Matching used the same characteristics as above (Table 2). Groups 1 and 2 were mutually exclusive with no participants on both metformin and statins. To create the insulin-only reference groups, participants reporting prior use of metformin or statin were excluded from matching pools. Two insulin-only groups were chosen to best match baseline characteristics for the metformin and statin groups. Twelve participants were included in both insulin-only reference groups.
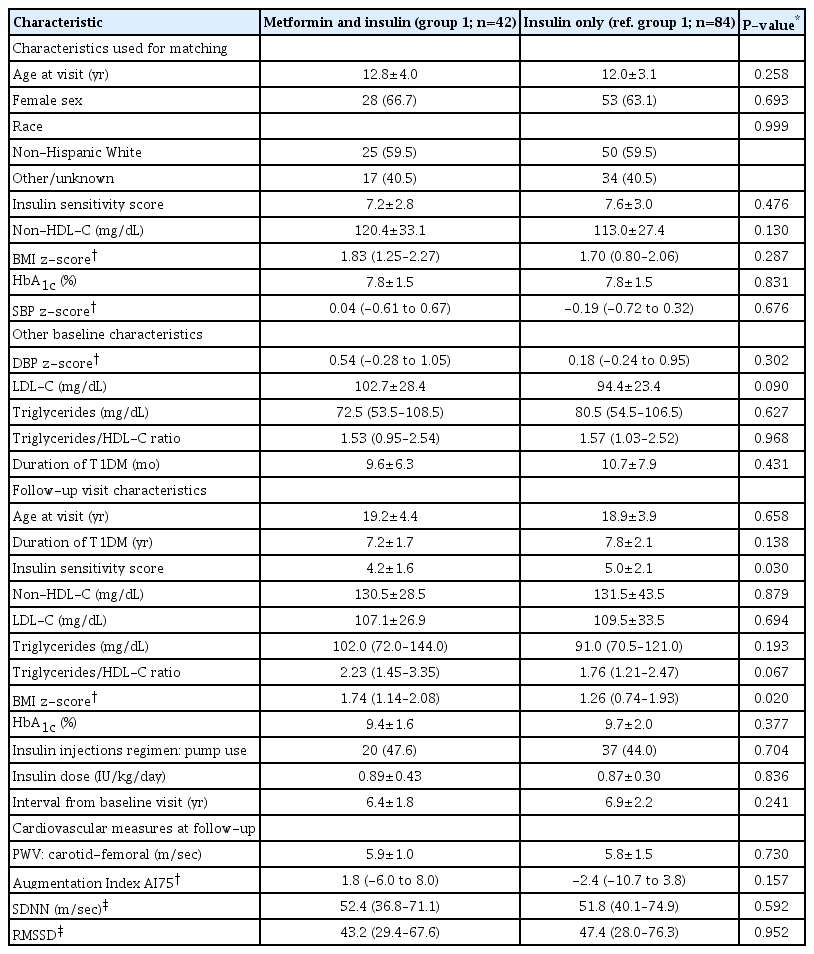
Baseline and follow-up visit characteristics for the group exposed to metformin (group 1) and the reference group 1
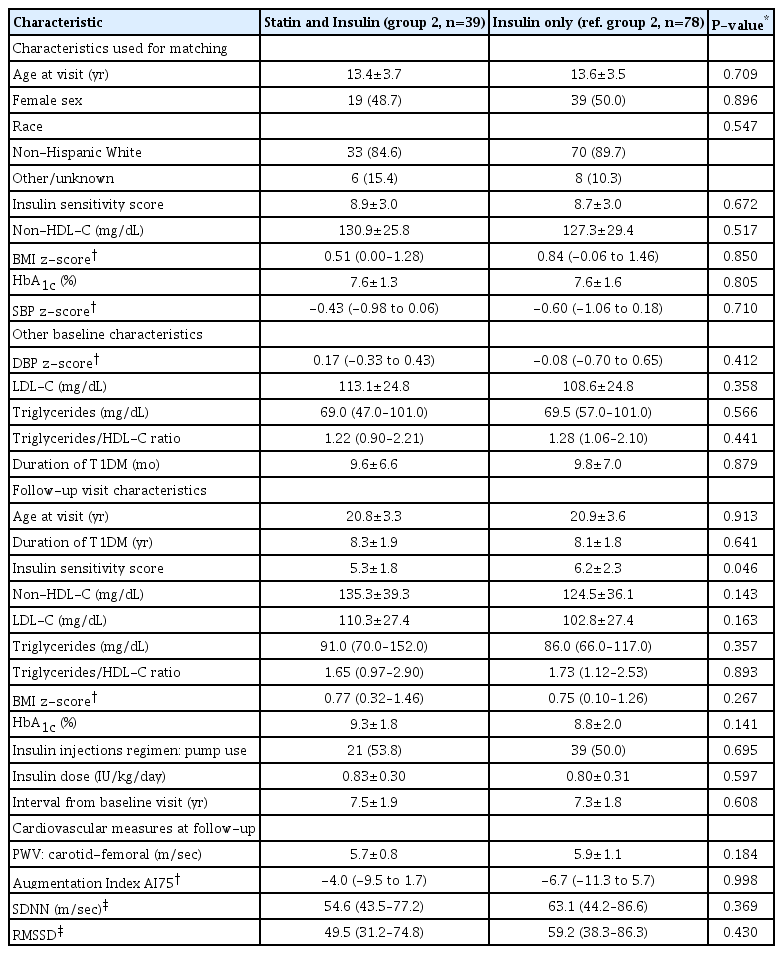
Baseline and follow-up visit characteristics for the group exposed to statin (group 2) and the reference group 2
Demographic and clinical characteristics of groups are presented as mean±SD or median (interquartile range) for continuous variables and count (%) for categorical variables. Associations between demographics, clinical characteristics, and surrogate measures of CVD between treatment groups were evaluated using chi-square test (categorical) or t-test or Wilcoxon rank-sum test (continuous). Adjusted linear regression models were used to evaluate differences in PWV between groups after adjusting for mean arterial pressure (MAP) and differences in AI75 between groups after adjusting for height. All statistical analyses were conducted using SAS ver. 9.4 (SAS Institute, Cary, NC, USA).
Results
1. Metformin treatment
Participants on metformin and insulin (group 1, n=42) were well matched with participants on insulin only (reference group1) at the baseline visit. Baseline characteristics of the groups are shown in Table 1.
Follow-up characteristics and surrogate measures of CVD obtained after an average follow-up of 6.7±2.1 years post baseline were compared between treatment and reference groups (Table 1). No differences were detected between participants on insulin plus metformin (group 1) and those on insulin only (reference group 1) in age, T1DM duration, non-HDL-C, LDL-C, and HbA1c. However, participants in group 1 had significantly higher median BMI z-score (1.74 [1.14–2.08] vs. 1.26 [0.74–1.93], P=0.020) and significantly lower IS score (4.2±1.6 vs 5.0±2.1, P=0.030) compared to reference group 1.
For surrogate measures of CVD, participants on metformin and insulin were not different than reference group 1: PWV was 5.9±1.0 m/sec vs. 5.8±1.5 m/sec, P=0.730. Median AI75 was 1.8 (-6.0 to 8.0) vs. -2.4 (-10.7 to 3.8), P=0.157. Median SDNN was 52.4 (36.8–71.1) vs. 51.8 (40.1–74.9) m/sec, P=0.591; and median RMSSD was 43.2 (29.4–67.6) vs 47.4 (28.0–76.3), P=0.952. These results did not substantially change after adjusting for MAP (PWV) and height (AI75) (data not shown).
2. Role of statin treatment
Participants on insulin plus statins (group 2, n=39) were well matched with the group exposed to insulin only (reference group 2) at the baseline visit. Baseline characteristics of these 2 groups are shown in Table 2.
Follow-up characteristics and surrogate measures of CVD were compared at the follow-up visit after an average of 7.4±1.9 years. No significant differences were observed between participants on statins and insulin (group 2) and those on insulin only (reference group 2) for age, duration of diabetes, median BMI z-score, non-HDL-C, LDL-C, and HbA1c. However, group 2 had a significantly lower IS score (5.3±1.8 vs. 6.2±2.3, P=0.046) than reference group 2 (Table 2).
For surrogate measures of CVD, participants on statins and insulin (group 2) were not significantly different from Reference group 2. PWV was 5.7±0.8 m/sec vs. 5.9±1.1 m/sec, P=0.184; median augmentation index AI75 was -4.0 (-9.5 to 1.7) vs. -6.7 (-11.3 to 5.7), P=0.998; median SDNN was 54.6 (43.5–77.2) m/sec vs. 63.1 (44.2–86.6) m/sec, P=0.369; and median RMSSD was 49.5 (31.2–74.8) vs. 59.2 (38.3–86.3), P=0.430 (Table 2). These results did not substantially change after adjusting for MAP (PWV) and height (AI75) (data not shown).
Discussion
1. Metformin use
In our observational cohort study, contrary to our hypothesis, we found no significant association between use of metformin or statin medication and surrogate measures of CVD in youth with T1DM.
Previous studies found favorable changes with metformin for weight gain and total insulin requirements in youth with T1DM [22,26]. These studies indicate that metformin use is associated with improved IS in youth with T1DM. A randomized controlled trial (RCT) in children with T1DM found that 12 months of metformin improved vascular function, as measured by brachial artery ultrasound flow [27]. Metformin did not improve carotid/aortic media thickness, either because it does not impact vascular structure or because longer follow-up is necessary to observe changes in vascular thickness [27]. The REMOVAL RCT of 428 adults with T1DM found improvements in maximum CIMT after approximately three years of treatment with metformin. This result suggests that metformin might be beneficial in improving atherosclerosis in participants with T1DM [28].
Based on the favorable effects of metformin on IS and the association of IS with arterial stiffness, we hypothesized that metformin use would be associated with improved measures of arterial stiffness. However, in our study, the 42 participants who reported using metformin did not have favorable markers of arterial stiffness compared to their matched reference group that did not report metformin use. Furthermore, the IS score of participants that were exposed to metformin was significantly lower at follow-up than was that of the group of participants that never used metformin. One possible explanation for this lack of association is that, even though participants who were exposed to metformin were well matched and had similar BMI z-scores at baseline to the nonexposed group, they gained more weight during follow-up than participants in the control group. Participants who were started on metformin by their primary care providers between baseline and follow-up visits may have had poorer glycemic control or gained a significant amount of weight and required high doses of insulin for T1DM management. SEARCH was an observational study, and the above information is missing from the database.
2. Statin use
We also examined the impact of statin use on surrogate CVD markers, as dyslipidemia is a major pathogenic mechanism tying type 1 diabetes and low IS with increased CVD risk. The prevalence of dyslipidemia in youth with T1DM varies between 3% and 18% and tends to persist over time [1,29,30]. Multiple studies have demonstrated that obesity, low IS, and glycemic control increase dyslipidemia risk in youth with T1DM [31]. Individuals with T1DM and low IS have higher atherogenic lipoprotein profiles characterized by higher LDL-C, total cholesterol, and TG [32]. However, a study showed that improved adiposity over time has a limited effect on dyslipidemia in youth with T1DM [33]. In the ancillary SEARCH Case Control study, 512 children with T1DM had lower small-density LDL-C (P<0.001) and higher apo-lipoprotein B (Apo-B) (P<0.0001) than 188 healthy participants [34], irrespective of glycemic control. Another study found that youth with T1DM and high Apo-B had higher arterial stiffness (measured by PWV), indicating a relationship between Apo-B and CVD in youth with T1DM [35]. High LDL-C is also associated with increased CIMT, another surrogate measure of CVD [36]. High level of LDL-C in youth with T1DM is associated with increased arterial stiffness over time [7].
Few RCTs have examined the use of statin medications in youth with T1DM. The largest was published by Marcovecchio et al. [37] In their study, even though statin use significantly decreased levels of total, LDL, and non-HDL cholesterol and TG after a median follow-up of 2.6 years, it had no effect on CIMT. A smaller crossover study found an LDL-C reduction of 29±20 mg/dL after 12 weeks of atorvastatin treatment [38] with good tolerance. Another trial randomized 42 children with T1DM to atorvastatin 20 mg daily or placebo for 6 months and found significant improvements in LDL-C and Apo-B without major adverse events [23]. These studies indicate that, although statins are effective in improving dyslipidemia after short treatment duration, longer follow-up studies are needed to determine if they also improve surrogate measures of CVD in youth with T1DM.
In our cohort, a subgroup of 39 participants with T1DM was treated with statins in addition to insulin. They did not have significantly different TG, non-HDL cholesterol, or LDL-C at follow-up than did the group that not take statins, which is unusual. Furthermore, the mean LDL-C was 110.3±27.4 mg/dL, which was above the recommended American Diabetes Association target of LDL-C 100 mg/dL [39]. This observation strongly suggests that statin dose and/or compliance with medication were inadequate, or that some participants had statin intolerance. However, we did not have data on LDL-C levels at treatment, duration and dose of treatment, or medication compliance of participants to make definitive conclusions. Another possible explanation for the lack of difference in lipids between these groups was that those on statins also had worse IS at the follow-up visit since this contributes to dyslipidemia.
3. Limitations and strengths
Limitations of our study include the observational design with nonrandomized exposure to metformin or statins. We have no information on what prompted participants' physicians to initiate treatment with metformin or statins, although we attempted to match for potential factors that could have affected provider decision making. We had no information on clinical variables (glycemic control, BMI z-score, or lipid levels) at the time of metformin or statin initiation. Another limitation is the lack of information about the duration of treatment with metformin or statins, participant compliance, and doses used, as well as information on exercise and puberty status. We used a validated formula to estimate IS. This is not the gold standard for measuring IS, but we previously validated the formula with insulin clamp studies and believe it is a good surrogate marker [25]. Our study included small numbers of participants treated with statins or metformin, and we had limited statistical power to detect differences. We would have needed sample sizes approximately twice as large to achieve statistically significant observational results. Also, the majority of people in the study was non-Hispanic whites, limiting the generalizability of our results, given racial disparities in CVD risk factors. Our study was not originally designed to address these questions; however, our cohort reflects real-life conditions, given that the majority of youth with T1DM is not treated with metformin or statin medications. Finally, another limitation is that we did not have baseline measurements for arterial stiffness or HRV to detect potential changes over time. However, our groups were matched for most CVD risk factors associated with arterial stiffness and HRV at baseline, which acted as surrogate markers.
Strengths of our study include a well-characterized cohort of individuals matched at baseline for multiple factors that contribute to CVD risk such as age, sex, race, IS score, non-HDL cholesterol, BMI, HbA1c, and SBP. We were also able to investigate associations between use of metformin and statins and well-established surrogate markers of subclinical CVD such as arterial stiffness and HRV in addition to measurements of IS and dyslipidemia.
4. Conclusions
In summary, the inconclusive results from our observational study do not suggest that metformin or statin improved cardiovascular outcomes in youth with T1DM. However, given that our study was observational, and we did not have information on baseline surrogate CVD measures, further studies are needed. Well-designed RCTs with longer follow-up and CVD endpoints such as arterial stiffness, HRV, and CIMT are needed to further investigate the effects of medications that improve IS and dyslipidemia on surrogate measures of CVD in youth with T1DM.
Notes
Ethical statement
This study was reviewed and approved by local institutional review boards at all SEARCH sites, and all participants provided written informed consent or assent (plus parental consent) prior to each visit.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
The SEARCH for Diabetes in Youth Study is indebted to the many youth and their families and their health care providers, whose participation made this study possible.
SEARCH for Diabetes in Youth is funded by the Centers for Disease Control and Prevention (PA numbers 00097, DP-05-069, and DP-10-001) and supported by the National Institute of Diabetes and Digestive and Kidney Diseases.
Site Contract Numbers: Kaiser Permanente Southern California (U48/CCU919219, U01DP000246, and U18DP002714), University of Colorado Denver (U48/CCU819241-3, U01 DP000247, and U18DP000247-06A1), Children’s Hospital Medical Center (Cincinnati) (U48/ CCU519239, U01 DP000248, and 1U18DP002709), University of North Carolina at Chapel Hill (U48/CCU419249, U01 DP000254, and U18DP002708), University of Washington School of Medicine (U58/CCU019235-4, U01 DP000244, and U18DP002710-01), Wake Forest University School of Medicine (U48/CCU919219, U01 DP000250, and 200-2010-35171).
The authors wish to acknowledge the involvement of the South Carolina Clinical & Translational Research Institute, at the Medical University of South Carolina, NIH/National Center for Advancing Translational Sciences (NCATS) grant number UL1 TR000062; Seattle Children's Hospital and the University of Washington, NIH/NCATS grant number UL1 TR00423; University of Colorado Pediatric Clinical and Translational Research Center, NIH/NCATS grant Number UL1 TR000154; the Barbara Davis Center at the University of Colorado at Denver (DERC NIH grant number P30 DK57516); the University of Cincinnati, NIH/NCATS grant number UL1 TR000077; and the Children with Medical Handicaps program managed by the Ohio Department of Health. This study includes data provided by the Ohio Department of Health, which should not be considered an endorsement of this study or its conclusions. Dr. Gourgari has support from a KL2: Award Numbers KL2TR001432 and UL1TR001409 from the National Center for Advancing Translational Science.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases.