Introduction
The incidence of thyroid malignancy has been increasing in adults, most rapidly in Korea [1]. Currently, thyroid cancer is the most common cancer in young adults and adolescents in Korea [2]. Many factors have been suggested to contribute to this rise in incidence. While environmental and genetic factors can affect the incidence of thyroid cancer, improved detection via advanced imaging techniques is regarded as the main factor responsible for the rise in incidence of small thyroid cancers [3,4]. Ahn et al. [1] suggested that thyroid cancer screening has increased detection of papillary thyroid cancers in Korea. Since thyroid screening in Korea is conducted in individuals older than 20 years, the factors contributing to the rise of thyroid cancer incidence in adolescents are unknown.
Thyroid nodules are infrequent in pediatric populations, occurring in only 0.2%ŌĆō5% of these individuals [5-7]. However, compared with adults, thyroid nodules are more often malignant in pediatric populations (up to 26% of all nodules). Moreover, the incidence of thyroid cancer in the pediatric population seems to be increasing [8-10].
Few reports have investigated thyroid nodules and cancer in pediatric populations. Moreover, reports about the incidence of thyroid cancer in pediatric patients with thyroid nodules in Korea are rare [11-13]. In this study, we aimed to determine the prevalence and clinical findings of thyroid cancer in thyroid nodules and to compare malignant and benign nodules in a Korean pediatric population.
Materials and methods
1. Subjects and methods
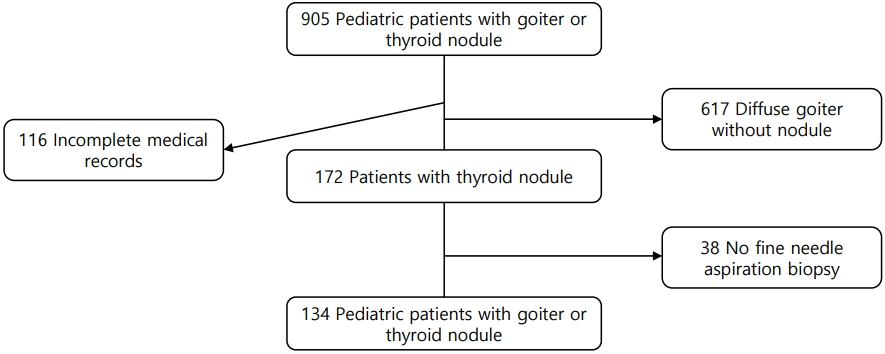
We investigated the medical records of 905 patients aged less than 18 years who had a goiter, thyroid nodule, thyroid mass, or thyroid cancer and who had visited St. Vincent's Hospital or Bucheon St. Mary's Hospital between January 2006 and December 2015. One hundred sixteen patients were excluded due to incomplete medical records, and another 617 were excluded because they had a diffuse goiter without a nodule. Of the remaining patients, 38 had not undergone ultrasonography-guided-fine needle aspiration biopsy (FNAB); therefore, 134 patients were included in the present analysis (Fig. 1).
FNAB was not performed for some patients (38 patients who were excluded) due to the following reasons: cystic nodule (n=8), small nodule (<1 cm) with little change in size during more than 1 year of follow-up (n=6), small single nodule with benign nature in ultrasonography (US) findings (n=8), initial operation without FNAB due to large size (n=3), or no description about the reasons and follow-up duration less than 1 year (n=13). Lobectomy was performed for 3 of the patients who did not undergo FNAB because of large tumor size. The final diagnosis was nodular goiter in all 3 patients. Of the 38 patients, none had a cancer diagnosis in their medical records.
US and FNAB were performed by well-trained radiologists, and FNAB specimens were reviewed by qualified pathologists. We regarded positive FNAB findings as more than atypia of undetermined significance or a follicular lesion of undetermined significance [14].
Serum triiodothyronine (T3), free T4 (fT4), and thyroid stimulating hormone (TSH) levels were measured by a chemiluminescent microparticle immunoassay using an Architect i2000 analyzer (Abbott, Abbott Park, IL, USA). Serum anti-thyroid peroxidase antibody (TPO Ab) and antithyroglobulin antibody (Tg Ab) levels were measured by a chemiluminescent immunometric assay using an Immulite 200 analyzer (Siemens Healthcare Diagnostic Products Ltd., Llanberis, Gwynedd, UK). TSHR Ab level, considered to reflect thyrotropin binding inhibitory immunoglobulin level, were measured by an electrochemiluminescence immunoassay using a Cobase 411 analyzer (Roche Diagnostics GmbH, Mannheim, Germany). The reference values were as follows: T3, 0.58ŌĆō1.9 ng/mL; fT4, 0.7ŌĆō1.79 ng/dL; TSH, 0.35ŌĆō4.95 ╬╝IU/mL; TPO Ab, <30 IU/mL; Tg Ab, <40 IU/mL; and TSHR Ab, <1.75 IU/L.
This retrospective study did not require written informed consent, and all of the work in this study was approved by the Institutional Review Boards of St. Vincent's Hospital (VC14risi0059) and Bucheon St. Mary's Hospital (HC17RESI0073).
2. Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). Continuous variables are expressed as mean┬▒standard deviation. Continuous data were analyzed using Student t-test and Mann-Whitney U-test, whereas categorical variables were analyzed using the chisquare test or Fisher exact test. Logistic regression analysis was performed to identify the risk factors contributing to malignancy in patients with thyroid nodule. P-values of <0.05 were considered statistically significant.
Results
The study population included 113 female patients (84.3%) and 21 male patients (13.7%); the mean patient age was 16.1┬▒2.3 (8ŌĆō18) years. Thyroidectomy was performed in 36 patients, and total thyroidectomy was performed in 15 of the patients with cancer. Of the 134 patients, 24 (18.0%) were finally diagnosed with thyroid cancer, 20 (83.3%) of which were papillary cancer (PTC) and 4 (16.7%) of which were follicular cancer. No patient was exposed to radiation. FNAB initially revealed that the nodule was positive (more than atypia) in 34 patients of the 134 and gave positive results in 21 of the patients with pathological cancer. While 3 of the 24 nodules in patients with cancer were initially reported as benign on FNAB, they were eventually diagnosed as follicular cancer. One of the patients had a 3.5-cm solid mass with irregular margins and cervical lymphadenopathy. However, another patient had a mass less than 1 cm in diameter and no calcification with multiple masses (more than 3 pieces) less than 1 cm. The third patient had a rapidly growing large mass with cervical lymphadenopathy. Otherwise, 13 of the patients who showed initially positive FNAB were finally diagnosed with nodular hyperplasia.
We next compared clinical parameters in the 2 groups (malignant vs. benign). Thyroid function, nodule size, and nodule number were not different between the 2 groups. However, cystic nodules were more common in the benign group (Table 1) (P<0.001). Cervical lymphadenopathy and irregular nodular margins were also more common in the malignant group compared to the benign group (Table 1). Although some FNAB findings were discordant with the final diagnosis, 85.1% of the FNAB findings were concordant with the final diagnosis.
Discussion
In the present study, the incidence of thyroid cancer in Korean pediatric patients with thyroid nodules was 18%. This incidence is comparable to the reported worldwide prevalence of thyroid cancer in pediatric thyroid nodules of 20%ŌĆō26% [8,9]. Including patients who did not undergo FNAB, and assuming that these patients might have benign nodules, 24 of the 172 thyroid nodules (14%) were malignant in pediatric patients in the present study. This incidence is slightly lower than those reported for other countries. In Korea, the childhood thyroid cancer incidence increased 3 fold from 1999 to 2012 (0.5/100,000 to 1.7/100,000), based on Korea Central Cancer Registry [13]. In the United States and the United Kingdom, the incidence of thyroid cancer in pediatric populations also appears to be increasing [10,13]. Additionally, the proportion of thyroid cancer out of all childhood cancers increased from 4.4% in 1999 to 10.6% in 2012 [13]. Little is known about the factors responsible for this increasing incidence of thyroid cancer in pediatric populations, due to the low incidence of thyroid cancer [15]. One risk factor is prior radiation exposure, e.g., in patients whose primary malignancy was treated with radiation [16]. PTC is related to radiation exposure [17,18]. However, none of the patients in the present study had a history of radiation exposure. In adult patients in Korea, cancer screening tests might contribute to the increasing incidence of thyroid cancer. However, children do not undergo these screening tests. According to a recent study, the proportion of PTC has decreased in Korean pediatric patients with thyroid cancer [12]. Therefore, environmental or genetic factors might be risk factors of pediatric thyroid cancer [19-21].
Similar to other studies, PTC was the major cancer in the present study. PTC accounts for more than 90% of all childhood thyroid cancers [22-24]. In another study of pediatric thyroid cancer in Korea, the incidence of PTC was 93.3% [12]. PTC frequently presents as a thyroid nodule with cervical lymphadenopathy [12,22]. Lymphadenopathy and margin invasion are characteristics of malignant nodules, and the presence of these 2 findings was more frequent in cancer nodules than in benign nodules in our study.
In this study, FNAB findings were used to discriminate between benign and malignant nodules in pediatric thyroid cancer. The diagnostic performance of FNAB was similar to that of other studies, which have reported a sensitivity of 83%ŌĆō98% and a specificity of 70%ŌĆō92% [5,25]. The sensitivity of FNAB in our study was 87.5% and the specificity was 88.2%, which are comparable to other results. FNAB is the most reliable method for determining whether thyroid nodules are malignant or benign.
Our study raises the question of how FNAB can be used to optimally evaluate children with thyroid nodules. According to the 2015 American Thyroid Association guidelines, FNAB is not warranted for a nodule <1 cm when the patient does not have a history of radiation exposure or pathologic regional lymphadenopathy [26]. However, the size criterion is problematic in children because thyroid volume varies by age [27]. Therefore, US characteristics and clinical findings should be used to determine whether FNAB should be conducted [28]. Irregular margins, hypoechogenicity, abnormal cervical lymph nodes, and increased intranodular blood flow are more common in malignant nodules [27,29]. Of these findings, cervical lymphadenopathy and irregular margins were found to be more common in malignant nodules than benign nodules in the present study. We could not compare intranodular blood flow between the groups, since this parameter is rarely described in medical records. Pediatric guidelines recommend that US characteristics and clinical findings should be emphasized rather than nodular size alone [28].
Other reports have suggested that high TSH level is related to thyroid cancer in patients with thyroid nodules. Therefore, TSH suppression could be useful for evaluating thyroid nodules, as stated in some of the pediatric guidelines [28,30]. However, we did not observe any differences in TSH level between benign and malignant nodules in the present study.
On account of limited medical records, we could identify only 6 patients had family history of thyroid disease (one patient had grandmother with thyroid cancer, and the others were only described as thyroid disease family history) in the cancer group.
A limitation of the present study is that it included a retrospective review of medical records. Although patients from 2 different hospitals were included, the relatively small study population hindered the identification of significant differences in our analyses. Despite these limitations, this study reports the prevalence of malignancy in pediatric thyroid nodules and identifies clues for discriminating benign from malignant thyroid nodules in Korean pediatric populations.
In conclusion, the incidence of thyroid cancer in a Korean pediatric population was comparable to the reported worldwide incidence in pediatric populations with thyroid nodules. Papillary thyroid cancers are dominant in Korean pediatric populations but are less prevalent than in Korean adults. Cervical lymphadenopathy increases the risk of malignancy; as expected, FNAB was highly accurate in predicting malignant nodules.