The effect of first nocturnal ejaculation timing on risk and sexual behaviors of Korean male adolescents
Article information

Abstract
Purpose
This study evaluated the effect of first nocturnal ejaculation timing on risk and sexual behaviors of Korean male adolescents.
Methods
We analyzed data from the 10th edition of the Korea Youth Risk Behavior Web-based survey that was conducted with male high school adolescents in grades 10–12. The survey included 17,907 adolescents, and 10,326 responded their experience of first nocturnal ejaculation. Of these, 595 had their first nocturnal ejaculation in ≤grade 4 (“early puberty”) and 9,731 had their first nocturnal ejaculation in ≥grade 5 (“normal puberty”). We analyzed differences between these 2 groups in risk and sexual behaviors.
Results
Early first nocturnal ejaculation showed a positive association with sexual intercourse (odds ratio [OR], 3.27; 95% confidence interval [CI], 2.56–4.17), sexual debut at elementary school age (OR, 7.45; 95% CI, 5.00–11.10), and having had a sexually transmitted disease (OR, 6.60; 95% CI, 3.94–11.08). After a multiple logistic regression to adjust for socio-demographic variables, early first nocturnal ejaculation was still positively associated with sexual intercourse (OR, 2.73; 95% CI, 2.03–3.69), sexual debut at elementary school age (OR, 5.96; 95% CI, 3.47–10.22), and having had a sexually transmitted disease (OR, 5.17; 95% CI, 2.52–10.20). Early first nocturnal ejaculation was positively associated with alcohol consumption, smoking, and substance use. However, this was not statistically significant after adjusting for several socio-demographic variables.
Conclusion
There is a positive association between early nocturnal ejaculation and sexual behaviors in male adolescents. Proactive education about sexual behaviors is required for adolescents who reach sexual maturity early.
Introduction
Adolescents who experience early puberty are reported to show increased alcohol consumption1), smoking2), substance use3), and risky sexual behaviors2). There is an association between rapid physical maturity and violence, crime, illegal substance use, and early sexual intercourse4). To date, however, such studies for Korean male adolescent have been very rare.
The first visible change in male puberty is an increase in the size of the testicles to a volume of approximately 4 mL. However, because it is not easy to recognize changes in testicular volume and penis size, it is difficult to determine the onset of puberty in males. Therefore, there is a lack of data on changes in the age of puberty onset, and different studies have applied different methods for evaluating the start of puberty, causing difficulties in identifying risk and sexual behaviors related to pubertal development in male adolescents. Therefore, despite a large number of studies on the effects of early menarche on risk and sexual behaviors, there is relatively little research on the effects of early sexual maturity on risk and sexual behaviors in males.
Ego identity formation is incomplete in adolescents; therefore, they are more likely to be emotionally sensitive, express curiosity towards the opposite sex, and rebel against their parents than adults are. This period is also accompanied by rapid physical development and sexual maturation. Consequently, it is important time not only for physical sexual changes, but also for the formation of one's social and sexual identity5).
This study investigated the effects of first nocturnal ejaculation timing of Korean male adolescents on risk and sexual behaviors.
Materials and methods
1. Participants
This study used data from the tenth Korea Youth Risk Behavior web-based survey conducted in 2014. The Ministry of Education, the Ministry of Health and Welfare, and the Korea Centers for Disease Control and Prevention has conducted this self-administered web-based survey with middle and high school adolescents in grades 7–12 every year since 2005.
The 2014 survey was conducted with 74,167 adolescents from 800 schools: 400 middle schools and 400 high schools. Adolescents (n=72,060) from 799 schools participated in this survey. To minimize the standard deviations, regions were categorized as large cities, medium-to-small cities, and countries and they were reclassified to account for geographical accessibility, the number of schools, the size of the populations, the living environments, the smoking rate, and the drinking rate. The schools were divided into middle schools, general high schools, and specialized high schools, and a number of sample schools were selected based on city, province, size of the city, and whether the schools were male adolescents only, female adolescents only, or coeducational schools. After the sample schools had been selected, one class from each grade was randomly selected and every adolescent in that class was surveyed, with the exception of adolescents who were on long-term absences, handicapped children, and adolescents with dyslexia. Male high school adolescents who were in grades 10–12 were included in this study. Male adolescents who responded that they had not undergone first nocturnal ejaculation at the time of the survey were excluded from the study. Therefore, participants were 17,907 adolescents, and 10,326 (57.2%; 95% confidence interval [CI], 56.3%–58.1%) responded that they had experienced their first nocturnal ejaculation.
2. Methods
The survey was conducted during computer classes when Internet connections were available, and each computer was randomly assigned to adolescents who answered the questionnaire anonymously. Adolescents were then divided into 2 groups: the “early puberty” group, who experienced their first nocturnal ejaculation in grade 4 or earlier, and the “normal puberty” group, who experienced their first nocturnal ejaculation in grade 5 or later. First nocturnal ejaculation is known to begin in “sexual maturity rating” stage 3, or middle adolescence, and this pertains to an age of 13–14 years on average6). The mean age of first nocturnal ejaculation for Korean males is 12.6 years according to the eighth Korea Youth Risk Behavior Web-Based Survey conducted in 20127). We included participants 2 years younger than the national average age of first nocturnal ejaculation as a cutoff point to divide adolescents into 2 groups.
The 2 groups were then compared for experience of alcohol consumption; smoking; substance use including butane gas, glue, stimulants, and narcotics; and sexual behaviors including having sexual intercourse, sexual debut at an elementary school age, and having had a sexually transmitted disease. Finally, for socioeconomic background, living with both parents, parental education, family's economic status, and academic performance were also investigated.
Adolescents' living status was categorized as either “yes” or “no,” which indicated whether or not the adolescent was living with both parents. Parental educational levels were categorized as “less than high school graduation,” “high school graduation,” and “more than college graduation.” Academic performance was divided into “good,” “average,” and “poor.” Family's economic status was divided into “high”, “middle” and “low”. Both educational performance and family's economic status were assessed by adolescents' self-responses. If they did not respond to the question, they were treated as missing values.
3. Statistical analysis
The data were stratified because of the complex nature of the survey's design. Therefore, the survey's weights and design effects were considered during the statistical analysis to confirm the factors' effects. Participants' characteristics such as living with both parents, family economic status, academic performance, and paternal and maternal education were compared using a chi-square test. A multivariate logistic regression analysis was performed to analyze the risk factors based on the differences in adolescents' risk and sexual behaviors (adjusted for sociodemographic variables of paternal educational level, maternal educational level, living with both parents, academic performance, and household income). All statistical analyses were performed using IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA), and a P-value of <0.05 was considered statistically significant.
Results
1. Participants' characteristics
Of the participants, 10,326 responded that they had experienced their first nocturnal ejaculation. Of these, 595 (5.9%; 95% CI, 5.4–6.5) comprised the early puberty group and 9,731 (94.1%; 95% CI, 93.5–94.6) comprised the normal puberty group. There were 1,517 adolescents and 1,576 adolescents who did not provide a response for paternal education and maternal education, respectively. A higher percentage of adolescents who had experienced first nocturnal ejaculation in grade 4 or earlier responded that they were not currently living with both parents (P<0.001). There were no significant differences between the 2 groups in terms of parental education, family's economic status, and academic performance (Table 1).
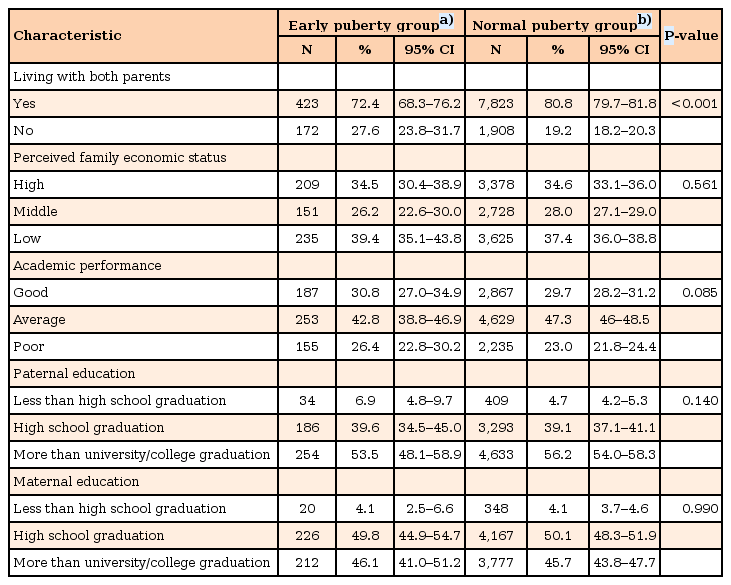
Subgroup characteristics defined by age at first nocturnal ejaculation
2. The effects of first nocturnal ejaculation timing on sexual behavior
Early first nocturnal ejaculation showed a positive association with having had sexual intercourse, sexual debut at elementary school age, and having had a sexually transmitted disease. This was true even after performing a multiple logistic regression to adjust for socio-demographic variables (Table 2).
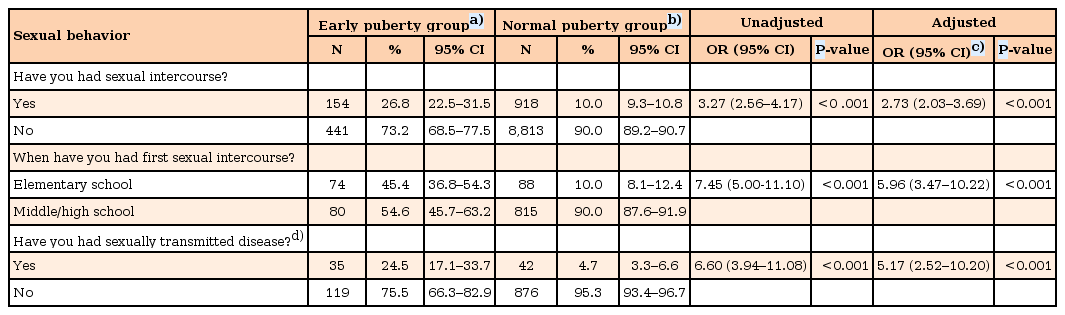
Association between sexual behavior and timing of first nocturnal ejaculation
3. The effects of first nocturnal ejaculation timing on risk behavior
Early first nocturnal ejaculation showed a positive association with experience of smoking, experience of alcohol consumption, and substance use. However, after performing a multiple logistic regression to adjust for socio-demographic variables, early first nocturnal ejaculation did not show any association with risk behavior (Table 3).
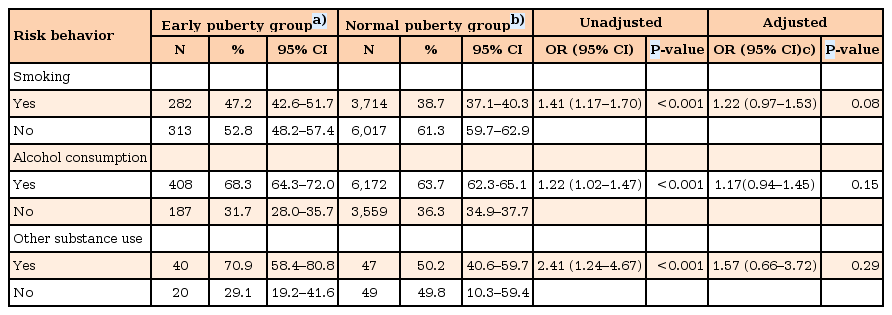
Association between risk behavior and timing of first nocturnal ejaculation
Discussion
This study asked male adolescents when they had their first nocturnal ejaculation, and used this to measure the timing of sexual maturity. Because males have no obvious marker of sexual maturity, such as menarche in women, age of first ejaculation is used as an estimation of sexual maturity, since it is evidence that spermatogenesis has commenced8). We found a positive association between early first nocturnal ejaculation and having had sexual intercourse, sexual debut at elementary school age, and having had a sexually transmitted disease.
A higher proportion of adolescents who had experienced early first nocturnal ejaculation were currently not living with both parents. According to a Korean study in 2011, the age of menarche in female adolescents who had grown-up in a single-parent household was 4–5 months earlier. The group who experienced earlier sexual maturity had higher levels of stress, and coming from a “broken family” was mentioned as one contributing factor9). There is also a hypothesis that interleukin-1 and corticotropin-releasing hormones play a role in this effect10).
In this study, there was no association between family's economic status and age of first nocturnal ejaculation. Consistently, a study of 4,116 adolescents in Switzerland found no association between socioeconomic state and timing of nocturnal ejaculation11). However, a United Kingdom study of 1,315 male adolescents revealed that socio-economic status was lower in male adolescents who experience puberty at age 11 years or younger compared to male adolescents with a later puberty onset (odds ratio [OR], 1.59; 95% confidence interval [CI], 1.09–2.31)2). Conversely, there is also research showing that a low socioeconomic status leads to chronic malnutrition and delayed pubertal development in both males and females12). Therefore, further research is required to address these conflicting findings.
In this study, a greater proportion of males who had their first nocturnal ejaculation in grade 4 or earlier had experienced sexual intercourse, and had sex at an early age. This was consistent with a study of male adolescents in Sweden: males who had their first ejaculation before 13 years had more sexual experience (adjust OR, 1.69; 95% CI, 1.11–2.57), and an earlier onset of puberty was associated with having sex before 15 years old (adjust OR, 3.48; 95% CI, 2.06–5.86)13).
Moreover, a study of 442 male students in Zimbabwe aged 12–18 years looked at the timing of first nocturnal ejaculation, testosterone level, and a pubertal development scale as measures of sexual maturity. The results showed a positive correlation between measures of sexual maturity and sexual behaviors, with first nocturnal ejaculation showing a stronger correlation than testosterone level and a pubertal development scale14). This demonstrates that male adolescents who experience first nocturnal ejaculation earlier are more likely to have had sex, and have sex at a younger age.
This study also showed a positive association between early first nocturnal ejaculation and having had a sexually transmitted disease. In a study of 17-year-old Swedish males, individuals who had their first ejaculation before being 13 years old (masturbation, 64.5%; nocturnal ejaculation, 35.5%), and those who had sex before being 15 years old were more likely to have had 5–10 sexual partners (OR, 2.07; 95% CI, 1.54–2.76), and also more likely to have had more than 10 sexual partners (OR, 2.57; 95% CI, 1.92–3.45). Sexually transmitted diseases were also reported to be more common in males who had sex before the age of 15 years (OR, 1.86, 95% CI, 1.22–2.84)13). We could not examine what mechanisms might link earlier puberty with adolescent sexual risk-taking. The temporal division between physical development and social maturity, social responsibility, and independence may be contributing factors15). Such divisions can be complicated when formal education on sexual risk-taking or discussions with parents are delayed as public institutions and parents fail to recognize earlier pubertal onset.
That is, the reason for the increased risk of sexually transmitted diseases in the group that reached sexual maturity sooner is thought to be because physical sexual contact occurred without proper sex education, and at a time when the individual's sexual identity had not been firmly established.
In Korea, students are educated on the differences between male adolescents and female adolescents in pubertal changes in grade 5 by a health education teacher or by their classroom teacher, while education on specific contraception methods and how to prevent sexually transmitted disease begins in grade 816). Since youths are reaching puberty earlier, youths need to receive sex education sooner. Specific sex education about contraception, pregnancy, and sexually transmitted disease using documents, visual material, and educational simulators is required, especially for youths who experience puberty earlier than their “normal” counterparts.
In this study, adolescents who had their first nocturnal ejaculation in grade 4 or earlier were more likely to consume alcohol, smoke, and use other harmful substances; however, after adjusting for socio-demographic variables, there was no statistical significance.
A study with 11- to 17-year-old adolescents in the United States (US) showed a higher frequency of smoking, alcohol consumption, and marijuana use among adolescents who reached sexual maturity earlier17). Moreover, a study of youths in Finland reported that an early age of first ejaculation was associated with earlier first experience of alcohol consumption, higher volume and frequency of alcohol consumption, and a higher risk of smoking and illegal substance use3).
Various hypotheses have been suggested to explain why early puberty onset acts as a risk factor for substance use18). One hypothesis is that the younger sexually mature youths experience functional brain changes earlier following the hormone surge of puberty, and this might cause behavioral maturation leading to earlier involvement in substance use19). A second hypothesis is that adolescents who reach sexual maturity earlier tend to socialize with older adolescents, who are similar to themselves in terms of external maturity, and are thereby at greater risk of exposure to substance use, which is typically more common in older youths20). A third hypothesis is the “maturation disparity hypothesis,” which proposes that younger sexually mature youths are ill-prepared and lack the cognitive and social ability to cope with their physical changes. In spite of rapid physical development, cognition and emotion remain immature; therefore, they lack the ability to control their affect and behavior21). Perhaps problematic behaviors such as substance use is a strategy to relieve this stress2223).
Looking at research on substance abuse in adolescents in the US and Korea, adolescents in the US showed far more substance use than adolescents in Korea (2 fold for cigarettes, 1.1 fold for alcohol, 6 fold for stimulants, and 42 fold for marijuana)24). In that study, a regression analysis was performed to examine factors related to “social learning theory,” such as the extent of substance use among friends, the attitudes of friends and parents towards substance use, and how parents and friends reacted when they found out about one's substance use. Specifically, 38.3% of alcohol-related behaviors and 30.1% of sedative and stimulant use in US adolescents was explained by social learning theory-related factors. Conversely, the same factors explained 57.0% of alcohol-related behaviors and 46.8% of sedative and stimulant use in Korean adolescents, suggesting that they were more likely to be influenced by social learning theory-related factors than US adolescents were. Given the low rate of alcohol consumption, smoking, and substance use in Korean adolescents compared to US adolescents, socioeconomic environmental factors may be more important than the timing of sexual maturation; however, further research is required.
This study has several limitations that must be addressed. Because this study analyzed the content of a self-reported, online questionnaire, there is the possibility of response error. The timing of first nocturnal ejaculation was used as a measure of sexual maturity; however, this was a subjective scale rather than an evaluation of pubertal development through a physical examination by an experienced specialist, or an objective biochemical marker like testosterone. Moreover, several males (7,581, 42.8%; 95% CI, 41.9–43.7) reported not having had their first nocturnal ejaculation. This was much higher than males in Indonesia (3%)25), and the US (17%)26). Kinsey et al.26) reported that there could be no experience of nocturnal ejaculation if the masturbation rate was high. Therefore, it is expected that there will be adolescents who were excluded even though they started puberty at an early age, thus limiting the generalizability of our findings.
In addition, it would be worthwhile investigating social and environmental factors such as parental interest in children, and extent of education at home and at school, in addition to analyzing affective problems and other factors that can affect sexual maturity.
In conclusion, this study found a positive association between early first nocturnal ejaculation and having had sexual intercourse, sexual debut at elementary school age, and having had a sexually transmitted disease. More specific sexual education that is implemented at an earlier age will help protect adolescents who reach sexual maturity at an early age from inappropriate sexual exposure and encourage them to engage in safer sexual behavior.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.