Introduction
The Diabetes Control and Complications Trial emphasized the need to lower glycated hemoglobin (HbA1c) levels to decrease the risk of chronic complication of diabetes1). HbA1c is the gold standard marker of glycemic control and a useful tool in preventing diabetic complications and educating patients in the clinical setting.
However, HbA1c has a number of limitations. HbA1c is a mean value of glycemia over 2-3 months and cannot capture daily glucose fluctuations2). It is also unable to distinguish between fasting plasma glucose and postprandial blood glucose (PBG)3). Recently, it has been suggested that postprandial hyperglycemia and glycemic excursions contribute to the risk of long-term complications in diabetes, increasing their importance in diabetes management4,5,6). Furthermore, HbA1c levels may be affected in patients with anemia, hemolysis, transfusion, renal disease, liver disease, alcoholism, drug use, and genetic hemoglobin abnormalities7,8).
Wild et al.9) estimated the prevalence of diabetes for all age groups to be 4.4% by 2030 and predicted that if the prevalence of obesity increased, the number of diabetics would be much higher than the estimated value. Thus, it is important to detect individuals with prediabetes who are at high-risk for type 2 diabetes mellitus (T2DM) and with undiagnosed diabetes, so that they receive appropriate early management10).
The three major fundamental components of metabolic disturbances in diabetes are fasting hyperglycemia, postprandial hyperglycemia, and acute glucose fluctuations6). According to previous studies, postprandial hyperglycemia and glycemic excursion are associated with cardiovascular disease11,12,13). Frequent checking of self-monitored blood glucose (SMBG) levels was used to evaluate postprandial hyperglycemia and variation in blood glucose levels14). However, this has limitations in reflecting glucose fluctuations precisely. Continuous glucose monitoring systems (CGMSs) are considered the gold standard for assessing glycemic excursion, but are quite expensive and invasive for wide application14,15). The compound 1,5-anhydroglucitol (1,5-AG) is a glucose analog that declines in hyperglycemic subjects. Recent studies have shown that 1,5-AG is reflective of PBG, glucose excursions, and short-term glucose status8,11,14). The Food and Drug Administration has recently validated 1,5-AG as a marker of short-term (2-3 weeks) glucose control status2,16).
The purpose of this study was to assess the clinical utility of 1,5-AG in early diabetes detection in patients with prediabetes status by comparison with HbA1c in overweight and obese (OWOB) children.
Materials and methods
1. Study population
This study was approved by the Institutional Review Board of Konkuk University Medical Center, Seoul, Korea (IRB No.: KUH1090036). The need for informed consent was waived. In total, 74 participants diagnosed with OWOB (body mass index [BMI] z-score Ōēź1.04, same as the 85th percentile) or diabetes were enrolled between August 2011 and January 2015 at Konkuk University Medical Center. The subjects (44 girls, 30 boys) were 14.3┬▒3.6 years of age and were classified into two groups: OWOB and diabetes. The OWOB group included patients who were overweight (1.04ŌēżBMI z-score<1.65, n=12) or obese (BMI z-scoreŌēź1.65, n=15) by 2007 Korean National Growth Charts17), and the diabetes group included patients who were type 1 diabetes mellitus (T1DM, n=26) or T2DM (n=21). The exclusion criteria included acute or severe chronic diabetes, severe comorbid disorders, and other acute illnesses that affected blood glucose. No subject had anemia, chronic kidney disease, or liver failure, and none were pregnant.
2. Biochemical measurement
Measurement of serum glycemic markers was performed as follows: plasma AG concentrations were measured using an enzymetric colorimetric assay (Kyowa Medex, Tokyo, Japan). And, HbA1c was assayed by high-performance liquid chromatography using Varaiant TM II turbo (Bio-Rad Laboratories, Hercules, CA, USA).
3. The criteria of HbA1c and 1,5-AG
According to previous study, the level of HbA1c for assessing impaired glucose tolerance (IGT) is 5.5%. And HbA1c>8% is usually considered to indicate poorly controlled diabetes18). Thus, we divided the subjects into three groups by HbA1c: <5.5%, 5.5%-8%, and >8%. The relationship between 1,5-AG and HbA1c was compared depending on this classification.
To determine the reference value of 1,5-AG, we followed previous studies. Kim and Park19) suggested that diabetes subjects with low 1,5-AG (<10 ┬Ąg/mL) were more prone to diabetic complications than those with high 1,5-AG (Ōēź10 ┬Ąg/mL). In another population-based cohort study in Japan, 23.1 ┬Ąg/mL was determined as the cutoff value of nondiabetic reference subjects20). Thus, we accepted 10 ┬Ąg/mL as the lower cutoff, and 23.1 ┬Ąg/mL as the upper cutoff value of 1,5-AG.
4. Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). Descriptive statistics are presented as mean┬▒standard deviation or proportions. Student t-test and one-way analysis of variance (ANOVA) were used to compare the mean values of variables. Logarithmic transformation of the 1,5-AG values was performed to assess the linear correlation between logarithmic transformed 1,5-AG values (ln [1,5-AG]) and HbA1c. We compared 1,5-AG with HbA1c using the Pearson correlation test. P-values<0.05 were considered to indicate statistical significance.
Results
1. Comparison of clinical parameters between the OWOB and diabetes groups
The clinical characteristics of the subjects are presented in Table 1. The subjects were composed of two groups: the OWOB (n=27; overweight:obese, 12:15; 36.5% of all subjects) and diabetes (n=47; T1DM:T2DM, 26:21; 63.5% of all subjects) groups.
In OWOB group, the mean age was 12.6┬▒2.9 years, the HbA1c was 5.5%┬▒0.3%, and the 1,5-AG was 31.1┬▒10.1 ┬Ąg/mL. In Diabetes group, the mean age was 15.3┬▒3.5 years, the levels of HbA1c was 8.9%┬▒2.7%, and the 1,5-AG was significantly lower than OWOB group as 7.4┬▒7.3 ┬Ąg/mL. The mean duration of diabetes was 3.3┬▒3.0 years.
The mean age of the OWOB group was 12.6┬▒2.9 years, younger than that of the diabetes (15.3┬▒3.5 years). The levels of HbA1c and glucose were significantly lower, whereas 1,5-AG was higher in the OWOB group than in the diabetes group (31.1┬▒10.1 ┬Ąg/mL vs. 7.4┬▒7.3 ┬Ąg/mL, P<0.001). The HbA1c of the OWOB group was 5.5%┬▒0.3%, and that of the diabetes group was 8.9%┬▒2.7%. The mean duration of diabetes was 3.3┬▒3.0 year.
The subjects were divided into 3 subgroups according to HbA1c: <5.5%, 5.5%-8%, and >8%. The patient's characteristics and the average values of the clinical parameters (age, gender, BMI z-score, and laboratory findings: glucose, lipid panel, and creatinine) were assessed using ANOVA and are presented in Table 2. Among them, the differences in HbA1c, glucose, and 1,5-AG were significant (P<0.001).
2. Distribution of 1,5-AG and the correlation between 1,5-AG and HbA1c
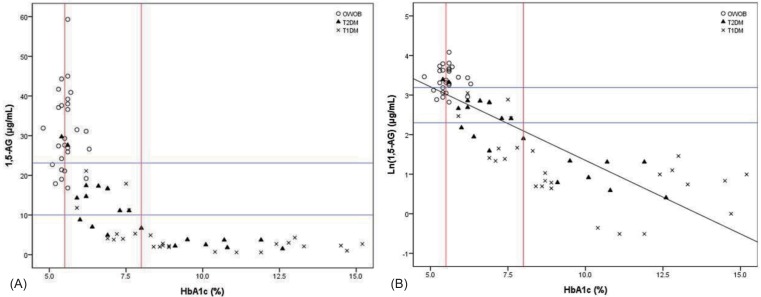
Most of the subjects with HbA1c<5.5% were in the OWOB group, except one who had well-controlled T2DM. This group showed substantial variation in 1,5-AG (17.9-44.3 ┬Ąg/mL), and had no correlation between 1,5-AG and HbA1c levels. For HbA1c>8%, all subjects were diabetics and none of the OWOB were included. The 1,5-AG levels were 2.4┬▒1.1, in the range of 0.6-4.9 ┬Ąg/mL, and also 1,5-AG did not correlate with HbA1c. However, for the HbA1c range of 5.5%-8%, each 1,5-AG was distributed more widely in the range of 3.8-59.3 ┬Ąg/mL, and correlated significantly with HbA1c (r=-0.736, P<0.001).
Fig. 1A shows the distribution of 1,5-AG according to HbA1c levels. The relationship between ln (1,5-AG) and HbA1c is shown in Fig. 1B. 1,5-AG was negatively correlated with HbA1c in the entire subject (r=-0.822, P<0.001), as it was in the diabetes group (r=-0.719, P<0.001). However, the 1,5-AG levels in the OWOB group had a wide range (16.8-59.3 ┬Ąg/mL) and were not correlated with HbA1c (Table 3). For HbA1cŌēż8%, ln (1,5-AG) was inversely correlated with HbA1c (r=-0.746, P<0.001). Among the diabetes in this range, 1,5-AG levels were <10 ┬Ąg/mL in nine subjects and Ōēź10 ┬Ąg/mL in 14 subjects. The 1,5-AG levels in the latter group increased, up to 29.7 ┬Ąg/mL, close to the normal range.
Discussion
1,5-AG is a six-carbon monosaccharide, the 1-deoxy form of glucose, that was first discovered in 188816,21). Because of its structural similarity to glucose, absorption of 1,5-AG is competitively inhibited by glucose in the proximal tubule if the renal threshold for glycosuria (generally>180 mg/dL in serum glucose) is reached8,21), after which levels of 1,5-AG in serum decrease rapidly8,21). Thus, patients with diabetes usually have markedly lower 1,5-AG levels than the healthy population22). The reported 1,5-AG range is quite wide, 0.49-110 ┬Ąg/mL, and the intra- and interassay coefficients of variation are small23). The sensitivity and specificity of 1,5-AG has been reported as being superior to HbA1c and fructosamine, respectively, and is 84.2% and 93.1% when the cutoff of the 1,5-AG concentration is determined as 14 ┬Ąg/mL24,25).
The amount of 1,5-AG is generally maintained at approximately 500-1,000 mg in total23). This originates mainly from food (4.4 mg/day), whereas its biosynthesis only provides a small source (~0.5 mg/day)26); 1,5-AG is balanced by urinary excretion, and its renal reabsorption is ~99.9%16). However, it can be affected by medications, diet, age, gender, race, and various pathological conditions (renal disease, liver disease, gastrectomy state, and cystic fibrosis)19). 1,5-AG is derived mainly from food and is influenced by diet and some medications19). The major food source is soy, and a small amount is included in rice, meat, fish, fruit, vegetable, tea, milk, and cheese23). A previous study showed that 1,5-AG decreased with aging in both sexes, and was higher in males than in females27); 1,5-AG was also significantly higher in Asian and African patients than in Caucasians19,23).
1,5-AG is suitable for evaluating short-term glucose status, glucose excursions, and PBG and thus is suitable for use in monitoring strict glycemic control19,28). Because postprandial hyperglycemia is a known risk factor for cardiovascular disease, control of PBG is an important target in glycemic control11). Stettler et al.29) showed that 1,5-AG was an optimal indicator of the 2-hour PBG value. According to Schindhelm et al.30), 1,5-AG was significantly inversely correlated with PBG, and the strongest association was seen in the second week, compared with HbA1c, which is considered to reflect mean glucose levels over the last 3 months. Sun et al.14) analyzed the correlation between 1,5-AG and glycemic excursion, using CGMS, and 1,5-AG was more closely related to glycemic excursions than HbA1c. However, unlike SMBG or CGMS, 1,5-AG does not provide information about the peak timing of hyperglycemia19). Besides, in some patients, there is a discordance between 1,5-AG and other glycemic markers; the reason for this discordance is presently unknown31).
Recently, markedly increased T2DM, even in children, could lead to profound economic costs for diabetic care and managing complications related to diabetes, and the importance of identifying prediabetics has increased9,32). Thus, today, early detection of prediabetes and appropriate intervention in early diabetes are very important in preventing the progress of diabetes32). Several prospective studies showed that 5-year cumulative incidence of diabetes was 12%-25% in subjects with HbA1c between 5.5% and 6%33,34,35,36). Data from National Health and Nutrition Examination Survey indicated that the subjects with HbA1c between 5.5% and 6% were prone to impaired fasting glucose or IGT. Therefore, subjects with HbA1c between 5.5% and 6% should be initiated preventive intervention37). In this study, we decided a lower cutoff of HbA1c, 5.5%, for prediabetes.
In this study, we compared 1,5-AG with HbA1c, the "traditional" standard marker of glycemic control, in the OWOB and diabetes groups. The 1,5-AG levels were significantly inversely correlated with HbA1c 5.5%-8%. The 1,5-AG values of diabetes subjects overlapped with the OWOB group when HbA1c was Ōēż8%, whereas most of the poorly controlled diabetics (HbA1c>8%) had prominently low levels of 1,5-AG, and showed no correlation between 1,5-AG and HbA1c, and this result was consistent with a previous report on severely uncontrolled diabetes19). According to this, 1,5 AG was a valuable index in prediabetic obese children and relatively well-controlled diabetic patients with HbA1c between 5.5% and 8%.
As mentioned earlier, 1,5-AG might be a more valuable marker of a detailed glucose status for the segment with HbA1cŌēż8%. This may imply that 1,5-AG better reflects glycemic changes of prediabetes than HbA1c. It was previously reported that serum 1,5-AG concentrations were lower in nondiabetic subjects with a family history of T2DM than in those with no family history38). The level of 1,5-AG, while maintained within the normal range, was decreased in IGT subjects39). The proportion of this reduction was correlated with the degree of glucose tolerance impairment. 1,5-AG precisely detected slight glycemic changes promptly, even in the near-normoglycemic range40). Also, HbA1c, fasting glucose, and 1,5-AG were reported as good predictive factors of T2DM in obese patients32). Among them, HbA1c and 1,5-AG were strong predictive variables of prediabetes just before T2DM in insulin-resistant obese patients32). Therefore, we suggested that the level of 1,5-AG could play a role in the continuum of diabetes in obese subject with a HbA1c level of less than 6.5% with glucose fluctuations and postprandial hyperglycemia.
1,5-AG is a valuable index in the HbA1c range 5.5%-8% and it might be considered as an early glycemic control index in obese patients with HbA1c levels of more than 5.5%., such as IGT or insulin-resistant obese children. Also, 1,5-AG level assessments should be stressed as a supplementary tool for better compliance as well as improvement of short-term glucose control in diabetes management in relatively well-controlled diabetes patients with an HbA1c level of less than 8%.
This study had several limitations. First, it is a retrospective study based on past medical records. Second, the small sample size and short follow-up durations of diabetes were additional limitations. Third, we could not examine patient glucose variability or peak glucose levels by CGMS or SMBG and were unable to include patients with large glucose variability. However, we did not select specific patients, thus more accurately reflecting a realistic diabetic population. Further studies are needed for 1,5-AG to be recognized as an early glycemic marker in prediabetes.