Introduction
Precocious puberty (PP) is defined as the development of secondary sexual characteristics before the age of 8 years in girls and 9 years in boys1). Depending on the presence of central activation of the hypothalamic-pituitary-gonadal axis, PP may be classified as gonadotropin dependent, also known as true or central PP (CPP), or gonadotropin independent, also known as pseudo-PP or peripheral PP (PPP). In contrast to CPP in girls, for whom 90% of sexual precocity is idiopathic, the prevalence of organic central nervous system (CNS) lesions is higher in boys (40% to 90%)2,3). Thus, brain magnetic resonance imaging (MRI) scans should be performed to rule out organic CNS causes in all boys with PP.
Several studies have evaluated predictors to identify girls with possible organic CNS lesions4-6). The prevalence of organic CNS lesions in girls is much lower when puberty starts after the age of 64,7). However, there are concerns about the risk of missing CNS lesions by not imaging low-risk girls between the ages of 6 and 8 years. In a recent single-center cohort study of girls with precocious or early puberty (EP)6), 13 of 208 girls (6.3%) with precocious or EP but no other signs of CNS symptoms had a pathological MRI result. These girls were all older than 6 years, and 6 girls were 8 to 9 years old. There is no consensus on the appropriate age limit for performing brain MRI in these children. Although data on CNS abnormalities in boys with PP are available8), no data exist on the prevalence of CNS abnormalities in boys with EP, defined as the appearance of pubertal signs between 9 and 10.9 years of age. Thus, further investigation of clinical and biochemical characteristics related to CNS abnormalities in boys with PP or EP is needed.
Peripheral causes of PP in boys can be induced by intracranial human chorionic gonadotropin (hCG)-producing tumors2). Even though there may be no apparent lesions in the initial MRI, the endocrinologist cannot guarantee that lesions will not develop later during the follow-up.
We evaluated brain MRI findings in boys with testicular enlargement Ōēź4 mL before 10.9 years of age. We also analyzed the characteristics related to the detection of organic CNS lesions at diagnosis and the later development of lesions during follow-up.
Materials and methods
This study was approved by the Seoul National University Hospital Institutional Review Board (IRB No. 1212-023-449). We retrospectively reviewed the medical records of all boys referred to the Division of Pediatric Endocrinology and Metabolism of Seoul National University Children's Hospital for clinical signs of PP or EP between January 1995 and April 2012.
Onset and progression of pubertal signs (testis enlargement, voice break, and pubic hair), growth velocity in the past year, concurrent symptoms (headache, vomiting, diplopia, visual field defect, and enuresis), birth history (birth weight and gestational age), and previous illness (intracranial infection, tumor, hydrocephalus [HCP], and/or cranial irradiation) were recorded. All boys underwent a physical examination and pubertal staging by a pediatric endocrinologist. Height (cm) was measured twice to the first decimal place with a Harpenden stadiometer (Holtain Ltd., Crymych, Wales, UK), and weight (kg) to the first decimal place with a digital scale. BMI was calculated as weight (kg) divided by height squared (m2). Height, weight, and BMI z scores were assigned according to the 2007 Korean National Growth Charts9).
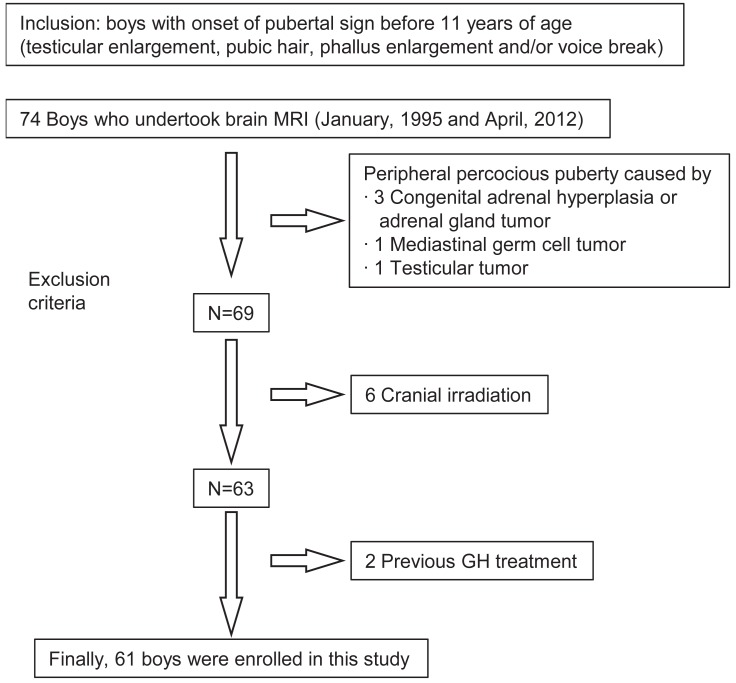
Bone age was assessed using the Greulich-Pyle scale. Plasma 17-hydroxyprogesterone and dehydroepiandrosterone sulfate concentrations were measured to exclude abnormal androgen secretion. Plasma thyroxin and thyroid-stimulating hormone (TSH) concentrations were measured to exclude hypothyroidism. Serum beta-hCG (╬▓-hCG) and alpha fetoprotein (AFP) concentrations were measured to screen for germ cell tumors (GCTs) and hepatoblastomas, and were measured by immunoradiometric assay kits (hCG: Riakey, Shin Jin Medics, Seoul, Korea; AFP: Beckman Coulter, Prague, Czech Republic). The sensitivity of the ╬▓-hCG and AFP assays was 0.23 mIU/mL and 0.2 IU/mL, respectively. Nonfasting venous blood samples were obtained to measure the concentrations of follicular-stimulating hormone (FSH), luteinizing hormone (LH), and testosterone. LH and FSH concentrations were measured using an immunoradiometric assay (Coat-A-count, Siemens, Malvern, PA, USA), and testosterone was measured by radioimmunoassay (Coat-A-count, Siemens). The detection limits were 0.15 mIU/mL, 0.06 mIU/mL, and 0.04 ng/mL, respectively, for LH, FSH, and testosterone. The gonadotropin-releasing hormone (GnRH) stimulation test was performed in 50 boys at the first visit. Serum LH and FSH levels were measured 0, 30, 45, 60, and 90 minutes after an intravenous bolus administration of LH-releasing hormone (100 g Relefact, Sanofi-Aventis, Frankfurt am Main, Germany). Boys with testicular enlargement before 9 years of age were diagnosed as having CPP if peak LH concentration was Ōēź5 IU/L10), or PPP if not. Boys with testicular enlargement between 9 and 10.9 years of age were defined as having EP11). We excluded 13 boys with PPP (n=5), history of cranial irradiation (n=6) and GH treatment (n=2) (Fig. 1).
No patients showed decreased growth velocity. All patients who were shown to have a pituitary lesion had a level of insulin-like growth factor-1 (IGF-1) that was compatible with their pubertal stage12).
Using the brain MRI results, we categorized the subjects into 3 groups. Group I included boys who had a pathological brain lesion related to pubertal development2); subgroup Ia had a newly diagnosed brain lesion, and subgroup Ib had a known brain etiology at the time of referral. Group II included those whose brain lesion had been reported in previous studies of PP patients but in which a causal relationship with PP was not proven2,13-15). Group III included those who had incidental brain findings not associated with puberty (subgroup IIIa) and those with normal brain MRI findings (subgroup IIIb).
1. Statistical analyses
Statistical analyses were performed using IBM SPSS ver. 19.0 (IBM Co., Armonk, NY, USA). Data are presented as median and range. The Mann-Whitney U test was used to compare groups. The Fisher exact test was performed to compare categorical variables that defined the most significant separation between groups. A chi-square test for trend was used to compare categorical variables between groups according to the age at pubertal onset. A probability value of P<0.05 was considered significant.
Results
All 61 boys were categorized into the 3 groups: CPP (n=23), PPP (n=8), and EP (n=30). The 31 boys with PP were categorized further according to age of onset of puberty; 0-2.9 years (n=2), 3-5.9 years (n=4), and 6-8.9 years (n=25) (Table 1).
1. Brain lesions related to CPP, PPP or EP
Group I included 23 boys who had a pathological brain lesion known to be related to pubertal development2) (Table 1). Group Ia included 12 boys who had a newly diagnosed brain pathology such as GCT (n=7), hamartoma (n=1), suprasellar arachnoid cyst (AC) (n=2), or pilocytic astrocytoma (n=2). All 7 boys with GCT were categorized initially as having PPP at the first GnRH-stimulation test. The results of biopsy were mature teratoma (n=3), immature teratoma (n=1), and choriocarcinoma (n=2). One patient did not have a biopsy, and the brain MRI diagnosis was mixed GCT or choriocarcinoma. Four of 7 boys were diagnosed with GCT after MRI evaluation at the first visit while 3 boys developed GCT later during follow-up (Table 2). Group Ib included 11 boys who had been diagnosed previously with the following brain pathology: optic glioma (n=1), astrocytoma (n=1), hamartoma (n=1), previous history of meningitis or encephalitis (n=3), HCP after intracranial hemorrhage (n=1), postoperative HCP caused by treatment for a ganglioma, teratoma, or retinoblastoma (n=3), and suprasellar AC (n=1). Group II included 10 boys who had a type of brain lesion that had not been proven definitively to cause puberty2,13-15). These included pituitary microadenoma (n=2), retrocerebellar AC (n=1), Rathke's cleft cyst (n=3), pineal cyst (n=2), empty sella syndrome (n=1), and neurofibromatosis (NF) stigmata (n=1). Group III included 28 boys who had incidental brain findings not known to be associated with puberty (group IIIa, n=6) and those boys with normal brain MRI findings (group IIIb, n=22). Group IIIa included 6 boys who had incidental brain findings such as prominent subarachnoid space (n=2), prominent perivascular space in the basal ganglia (n=1), focal high intensity in the white matter (n=1), a cystic lesion in the white matter (n=1), or a cyst in the choroidal fissure (n=1).
2. Factors related to pathological brain lesions in boys with PP or EP
In our study, which excluded other peripheral organic causes of PP (adrenal gland, testis, liver, or other sites), 7 of 8 boys with PPP were diagnosed with intracranial GCT (Table 1). Clinical and biochemical factors related to the presence of a pathological brain lesion were analyzed in the 53 boys with CPP or EP (Table 3). Boys with a newly diagnosed CNS pathology (group Ia) or those with a newly or previously diagnosed CNS lesion (group I) showed earlier pubertal onset, greater bone age advancement, and higher BMI z scores than those without a pathological lesion (group III, all P<0.05) or those with normal brain imaging (group IIIb, all P<0.01). The differences in height z scores (P=0.058) and the percentage of boys with neurological symptoms (P=0.056) between group Ia and group III were nearly significant. When we combined the group with newly diagnosed CNS pathology known to be related to puberty (group Ia) with the group with CNS pathology possibly related to puberty (group II), boys without such pathological CNS lesions (group III) had fewer neurological symptoms at diagnosis (P=0.047) and had a birth history of lower birth weight (P=0.012). Among the 28 boys with EP (excluding 2 boys with a previously diagnosed brain lesion), no significant characteristics were found to differentiate boys who had a newly developed brain lesion (n=7, groups Ia and II) from those who did not (n=21, group III).
3. Three patients who developed GCT during follow-up
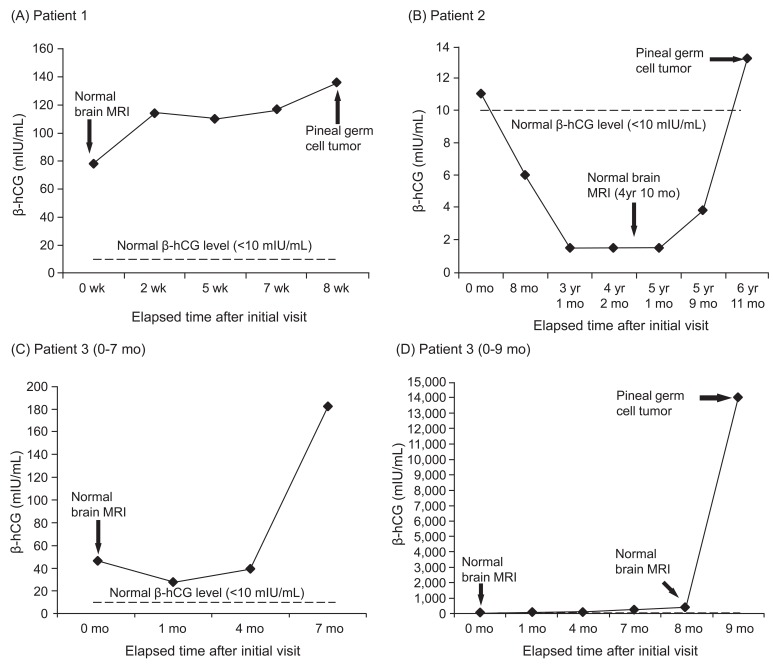
In the 25 patients with normal brain MRI findings at the initial evaluation, no boys with CPP or EP developed a pathological lesion during follow-up. However, 3 boys with PPP, who had elevated levels of serum ╬▓-hCG without an apparent CNS lesion at diagnosis, later developed a GCT in the pineal gland during follow-up (Table 2, Fig 2). The interval between the diagnosis of PPP and visible tumor detection was 2 months, 6 years 11 months and 9 months for the 3 boys respectively. Although patient 1 and patient 3 showed persistently elevated levels of ╬▓-hCG during follow-up, the second had fluctuating ╬▓-hCG levels. Patient 2 had a slightly increased level of ╬▓-hCG at the time of initial presentation (11 mIU/mL); this level returned to the normal range during follow-up but later increased again (13.2 mIU/mL) at the time when the visible tumor was detected (Fig. 2).
Discussion
The percentages of boys with a newly developed pathological CNS lesion related to puberty (group Ia) were 88% (7 of 8), 29% (4 of 14), and 4% (1 of 28) for PPP, CPP, and EP, respectively. Including previously diagnosed pathological CNS lesion (group Ib), the percentage were increased to 57% (13 of 23), and 10% (3 of 30) for CPP, and EP. The increase of percentage may be due to the fact that many patients with pathological brain lesions such as optic glioma, astrocytoma, hamartoma, HCP, suprasellar arachnoid cyst, and CNS infection were followed up in this tertiary referral university hospital. The percentages of boys with a brain lesion possibly related to puberty, for which a causal relationship has not been proven (pituitary microadenoma, Rathke's cleft cyst, retrocerebellar AC, pineal cyst, empty sella syndrome, and NF stigmata) were 17% (4 of 23) and 20% (6 of 30) for CPP and EP, respectively. Among boys with initially normal brain MRI findings, 3 boys who were diagnosed with PPP later developed a visible CNS lesion (all GCT) during the follow-up. Boys with a pathological brain lesion showed earlier onset of pubertal signs, greater bone age advancement, and higher BMI z score than those with idiopathic PP or EP.
Tumors in the pineal region cause PP by interrupting CNS inhibitory pathways to the hypothalamus. In boys, another mechanism involves secretion of ╬▓-hCG, which stimulates the Leydig cells of the testes because of the high structural similarity of LH and hCG. Intracranial hCG-secreting tumors do not usually cause PP in girls presumably because complete ovarian function cannot occur without FSH priming. Thus, an hCG-secreting GCT in boys may present as PPP unrelated to hypothalamic-pituitary-gonadal activation16-18). Occasionally, symptoms such as growth delay and enuresis related to endocrine dysfunction may not have a well-defined anatomic correlate, leading to a considerable delay in diagnosis19). PPP may also lack a visible tumor correlate18). Thus, even when a patient presents with normal neuroradiographic features at diagnosis, we propose that PPP warrants serial monitoring of ╬▓-hCG levels and/or brain MRI to detect an emerging intracranial GCT. However, no boys with CPP or EP with initially normal neuroradiographic features later developed a new intracranial lesion during follow-up.
The pathological CNS lesions responsible for CPP and PPP in our study were similar to those in previous studies20-23) (Table 4). The underlying disease of the youngest boy presenting with CPP in our study was a hypothalamic hamartoma, which was reported previously in a 7-month-old infant with PP24). Hypothalamic hamartoma was the most commonly identified CNS lesion in previous studies whereas in our study, optic glioma and obstructive HCP were the most common lesions in CPP patients. This may be due to the fact that many optic glioma and HCP patients were followed up in this tertiary referral university hospital. A total of 7 GCT cases were found in the PPP patients. According to Rivarola20), GCT was found in 5 of 18 patients (28%) with suprasellar and pineal tumors. Suprasellar and pineal tumors were found in 16 patients in this study. The ratio of intracranial GCT to suprasellar and pineal tumors was 7 of 16 (44%), which was high compared to previous study.
The possible association between PP and other brain lesions, including pituitary microadenoma4,6), Rathke's cleft cyst13), pineal cyst25,26), empty sella syndrome14), and NF stigmata in the absence of optic glioma15,27), have been described in previous PP case reports. AC may be related to PP regardless of the location of the tumor in the suprasellar area or in another area such as the retrocerebellar area distant from the hypothalamus28). Although it is not known whether this relationship is causative4,17), these lesions are not negligible and need to be monitored regularly because of the risk of size increments and possible pituitary hormone deficiencies.
The fact that 7 of 28 patients (25%) with EP (excluding 2 with previously diagnosed lesions) were newly diagnosed with a CNS lesion leads us to recommend brain imaging for boys with EP. When boys with PPP caused by a lesion of mediastinal, hepatic, adrenal, or gonadal origin were excluded, 7 of 8 boys were diagnosed with an intracranial hCG-secreting tumor at diagnosis or during follow-up. Thus, we believe it is reasonable to conclude that all patients with gonadotropin-independent PP at initial evaluation should be investigated thoroughly for an organic cause.
Pathological brain lesions can be predicted by earlier pubertal onset in boys with CPP, as previous studies have reported in girls2,4-6). Unlike previous reports6,8), in our study, basal LH or stimulated LH/FSH peaks did not differ significantly between boys with a pathological brain lesion and those without. Boys with a newly diagnosed brain lesion showed greater bone age advancement and higher BMI z score, reflecting progressive puberty and exposure to sex hormones; however, they were not taller than those without a brain lesion. When boys with PP or EP are too short for their stage of pubertal development, the physician must rule out a combined pituitary hormone (GH and/or TSH) deficiency possibly caused by an organic brain lesion20,29). However, there were no boys with pituitary hormone deficiency at diagnosis of PP or EP in our study, although screening was limited to IGF-1 level, the thyroid function test, and checking for normal growth velocity. We believe that the importance of all boys with PP or EP being evaluated for the presence of neurological symptoms suggesting a newly developed CNS lesion cannot be emphasized enough. In our study, boys without a pathological CNS lesion were more likely to have had a low birth weight; a previous report showed that low birth weight is related to early pubertal timing30).
In conclusion, three-quarters of boys with CPP and one-quarter of boys with EP had a newly or previously diagnosed brain lesion that needed to be treated and/or monitored regularly. Earlier onset of puberty, greater bone age advancement, and higher BMI z score indicate a greater chance of a pathological brain lesion in boys with CPP or EP. All boys with PPP, in whom an organic lesion may not be detected at diagnosis, should be evaluated thoroughly for the future emergence of a GCT.