Highlights
· Kabi International Growth Study was the largest, longest-running pharmaco-epidemiological study of recombinant human growth hormone (rhGH) use under real-world conditions. The overall results showed that rhGH is safe and increases both short-term height gain and adult height in children with growth hormone deficiency and multiple other short-stature conditions.
Introduction
After 1958, human growth hormone (hGH) extracted from cadaveric pituitary glands was used for hormonal replacement until that synthesized by recombinant technology became available in 1985 [1]. This authentic recombinant hGH (rhGH) for daily injections was synthesized in a modified strain of Escherichia coli and initially produced by Genentech as Protopin (South San Francisco, CA, USA) and KabiVitrum (Stockholm, Sweden) as Somatonorm, respectively [2]. KabiVitrum was subsequently acquired by Kabi Pharmacia in 1991 and then by Pharmacia & Upjohn in 1994; the latter was subsequently purchased by Pfizer (New York, NY, USA) in 2003 [3]. The Pfizer rhGH product was marketed under the brand name Genotropin. It was initially approved by regulatory authorities in Sweden in 1985 and in the United States (US) in 1987, but it was not marketed in the US until 1995 following the expiration of a 10-year marketing agreement between Genentech and Kabi [2]. After its approval in the US, medical authorities requested the conduct of a postmarketing surveillance study including 500 patients, initially termed the Kabi International Growth Study (KIGS). The "K" in the acronym "KIGS" stands for Kabi Pharmacia and was also used for the ongoing Pfizer International Growth Database.
KIGS was first established in 1987 under a survey guideline [4]. It later evolved to become an international, noninterventional (NI), phase 4, pharmaco-epidemiological study (Study A6281306 [87-052]) sponsored by Pfizer Inc. with the objectives of evaluating long-term safety and treatment outcomes in pediatric subjects who received Genotropin therapy as prescribed by physicians in real-world clinical practice settings around the globe [5]. Subjects were followed as long as KIGS investigator-physicians deemed it appropriate and as per the subject's/family's consent. Due to the NI nature of KIGS, no specific diagnostic or monitoring procedures were required, and epidemiological methods were used for the analysis of all collected data. Study enrollment was terminated on June 30, 2012, after 25 years.
Governance
There was a special interaction between Pfizer, the manufacturer of Genotropin, and the medical community based on a democratic structure with representatives from treating physicians within a country, forming a National Board. Additionally, representatives from each country formed an International Executive Board as the central owner/guardian of the database. From this Board, members were elected to form a smaller Strategic Executive Committee (SEC) consisting of international experts in the field of growth elected from the National Boards and expert representatives from Pfizer who guarded the process of analyzing and publishing results from KIGS after approval from the Boards. After 2002, members from the International Board elected into a Strategic Advisory Board (SAB) served as advisors to the Pfizer Endocrine Care, KIGS Medical Outcomes group [5] (Table 1).
Objectives
There were 4 primary objectives of KIGS [6], as follows: (1) assess the long-term safety of GH and GH treatment outcomes in subjects who were treated with Genotropin; (2) determine relationships between clinical status, dosage schedule, history of pretreatment with GH (as appropriate, if GH treatment were started before enrollment in KIGS), and response to Genotropin treatment; (3) develop a scientific foundation and clinical tools for individualized GH treatment of pediatric subjects and optimize their management throughout the course of GH treatment and their transition from pediatric to adult care; and (4) contribute to our knowledge of growth, growth disorders, and GH treatment of pediatric subjects through the exploratory analysis of captured study data.
Methods
As mentioned previously, KIGS was an international, multicenter, NI study open to all pediatric subjects with impaired growth or GH disorders who were treated with the Genotropin brand of rhGH both for indications approved by local regulatory agencies and for other indications deemed necessary by treating endocrinologists as part of their usual medical practice. This could include (but did not require) routine diagnostic procedures (e.g., bone-age imaging and blood samples to assess dosing adequacy and/or for monitoring for adverse events [AEs]), interviews, and questionnaires based on the clinical practice style and judgment of the individual KIGS investigator [6].
For the incorporation of patient data, informed written consent was given by legal guardians. Subjects were treated by participating KIGS clinician-investigators who collected and initially entered relevant subject data onto paper case report forms (CRFs) designed to document information relevant for both AEs and efficacy prior to September 2005. With the expansion of indications for the treatment of children with short stature beyond GHD, a multiplicity of disease-specific CRFs were designed. The paper CRFs were replaced in the US and, after April 2006, in all other countries, with electronic CRFs contained within an Internet-based platform known as endoKIGS, a password-protected data entry and management tool available to KIGS investigators [5]. Submitted data were abstracted from medical histories, physical examinations, and imaging/laboratory data obtained as part of routine visits and were related to safety and efficacy. Before any formal data analysis could be undertaken, the CRFs were subjected to quality control to detect any obvious formal errors using algorithms and with the involvement of the expert members of the SEC/SAB. The data-collection period could start before and continue during and after the conclusion of the Genotropin treatment. As the data collection was at the discretion of each individual investigator, the information collected could vary among investigators and, thus, may not have been obtained or, even if obtained, not necessarily submitted for a number of reasons, including failure to record data that were returned after the visit, e.g., bone ages and laboratory results. Collected data were subsequently anonymized and analyzed by the study investigators, in collaboration with Pfizer, to evaluate basic safety, treatment, and research outcomes as well as specific research questions [5].
For the purpose of structuring the various diagnoses, a KIGS Etiology Classification System was developed [7]. This formal coding system was based on the following principles: (1) the system should permit classification of all subjects; (2) there should be flexibility for incorporating new developments in etiologies and pathogenetic aspects; (3) the list of diagnoses should be clearly defined to avoid misclassifications; (4) the classification should follow one basic principle, e.g., nosology, etiology, pathogenesis, or symptomatology; (5) the system should be user-friendly; and (6) the system should serve the goal for which it is designed in an optimal fashion.
In KIGS, AEs were defined as all unfavorable changes in structure (as confirmed by signs), function (as confirmed by symptoms), or biochemistry (as confirmed by laboratory tests) occurring during the course of treatment. Whether or not a given AE was related to treatment with GH had to be evaluated in a second step. Serious AEs (SAEs) included those AEs that were life-threatening or fatal, resulted in permanent disability, required hospitalization, or involved malignancy [8]. The safety outcomes of interest included demographic characteristics; incidence rates of all reported, all-causality, and treatmentrelated AEs and SAEs, including neoplasms and death; study discontinuations due to AEs; general discontinuations from the study; and biochemical safety measures, such as insulin-like growth factor (IGF)-1 and insulin-like growth factor-binding protein 3. Treatment outcomes of interest included auxological data (height, height standard deviation score [SDS], height velocity, height velocity SDS, distance from or beyond genetic target height, adult height, and weight), pubertal status, bone age, and body composition. Lastly, research outcomes included the results of routine diagnostic procedures (e.g., blood tests) and interviews performed by investigators based on their specific research interests.
Data collected during the course of the study were analyzed after approval of the Boards and after detailed planning within the SEC/SAB by Pfizer statisticians, in collaboration with KIGS investigators, according to statistical analysis plans using well-accepted procedures in biostatistics and epidemiology. In general, continuous endpoints were summarized using descriptive statistics (means, standard deviations, medians, and minima and maxima often presented as whisker [box] plots), while categorical endpoints were summarized by frequencies and proportions [6].
Results
1. Descriptive and demographic data
Data from 83,803 subjects (58% of whom were male and 42% of whom were female, and covering 277,264 patient-years) were entered into the database [6,9]. All of these individuals were subjected to an analysis of safety. The 55,284 who were treated with Genotropin for ≥1 year were analyzed for their growth responses. Of the entire cohort, 62.2% were from Europe, 20.0% were from the US, 13.2% were from Asia, and 4.7% were from other parts of the world. Fifty-two countries participated in the study, of which the US, Germany, and Japan were the highest recruiters, enrolling 16,737 (20.0%), 11,488 (13.7%), and 10,525 subjects (12.6%), respectively.
Irrespective of the approval of a specific diagnosis by national authorities, information on patients with any diagnosis treated by physicians with Genotropin was incorporated into KIGS. In total, 150 different diagnoses were recorded [6,9]. The 5 most common etiologies for treatment in KIGS were idiopathic GHD, classical form (39,298 subjects [46.9%]); small for gestational age (SGA) (7,936 subjects [9.5%]); Turner syndrome (7,714 subjects [9.2%]); SGA/intrauterine growth restriction, cause unknown 6,101 subjects [7.3%]); and idiopathic short stature (ISS) (5,139 subjects [6.1%]). The mean duration of exposure was 3.8 years, while the longest duration of treatment was >18 years. Among all patients treated, the median initial GH dose depended on the underlying diagnosis and ranged, on average, between 0.17 mg/kg/wk for subjects with craniopharyngioma to 0.33 mg/kg/wk for those with chronic renal failure.
2. Safety data
KIGS investigators were asked to report all AEs observed. However, since reporting was voluntary, the submitted data, at least for non-severe AEs, are likely to be incomplete. Safety was evaluated in all GH-treated patients, and efficacy was evaluated in those who were treated for one or more years. A subgroup analysis of patients treated with GH for ≥5 years (of which 2 or more were during the prepubertal years) and who had reached their near-adult heights was performed. Over the course of KIGS, there were several specific publications (papers or KIGSBook chapters) on AEs according to diagnosis.
Among the entire KIGS cohort [9], 12,055 subjects (14.4%) reported 23,163 AEs, of which 2,638 (3.1%) were considered to be treatment-related by the investigator. Of the total, 3,108 subjects (3.7%) reported 3,981 SAEs; notably, 349 subjects (1.6%) had an AE that led to discontinuation of their Genotropin treatment, and 180 subjects (0.2%) received a dose reduction due to AEs. SAEs occurred in 3.7% of patients. The most frequently reported all-causality AEs were headache (987 subjects [1.2%]), scoliosis (514 subjects [0.6%]), and upper respiratory infection (474 subjects [0.6%]). The most frequently reported treatment-related AEs were headache (328 subjects [0.4%]), scoliosis (162 subjects [0.2%]), increased IGF-1 (146 subjects [0.2%]), and arthralgia (129 subjects [0.2%]). Finally, the most frequently reported SAEs (all-causality and treatmentrelated) were craniopharyngioma recurrence (151 [0.2%] and 42 subjects [0.1%], respectively), neoplasm recurrence (99 [0.1%] and 23 subjects [<0.1], respectively), scoliosis (91 [0.1%] and 43 subjects [0.1%], respectively), and recurrent cancer (91 [0.1%] and 26 subjects [<0.1], respectively) (Table 2) [6,9].
3. Discontinuations and deaths
Of the 83,803 total enrollees, 48,991 subjects (58.5%) withdrew from KIGS after a mean of 3.2 years of treatment [6,9]. Discontinuation occurred in 36,712 subjects (43.8%) because of normal height attained (5,665 [15.5%] of discontinuers), growth-plate fusion (4,753 [12.9%] of discontinuers), or the most frequent category of "other reasons" (10,363 [28.2%) of discontinuers). Other reasons for study discontinuation were related to the normal treatment process and included (1) height velocity diminishment or (2) change to another physician, KIMS enrollment (see below), or transference to a clinic for adults. Causes for discontinuation unrelated to the normal treatment process included patient/parent decision to stop, treatment noncompliance, loss to follow-up, moved to an unknown place, no more funds for GH, end of treatment trial, change to another brand of GH, AE, puberty, and other unidentified reasons [10]. Complete treatment discontinuation due to treatment-related SAEs occurred in 314 subjects (0.4%) while, in 98 (0.1%), there was a temporary treatment discontinuation and dose reduction (excluding subjects who died) [6,9].
There were reports of 280 deaths in KIGS during the course of the study. Most deaths were due to neoplasms (primarily in patients with medulloblastoma, other cranial tumors extracranial malignancy, and craniopharyngioma). The most common specified causes included neoplasm recurrence (benign, malignant, or unspecified), recurrent cancer, craniopharyngioma, new or recurrent brain neoplasm, illdefined disorder, cerebral hemorrhage, convulsion, glioblastoma, and pneumonia. Among 24 deaths registered as likely treatment-related, 20 were tumor-related, one was due to intracranial hemorrhage, and 3 had unspecified causes. Among the 5 patients who died of cerebral hemorrhage (1 reported as treatment-related and 4 reported as unrelated), 3 had GH deficiency (one each with craniopharyngioma, neurosecretory dysfunction, and congenital GHD, respectively), 1 had TS, and 1 had chronic renal failure [6,9].
Discussion
Unlike interventional clinical trials in which study populations are fairly homogenous as a result of specific enrollment criteria, KIGS was open to all pediatric subjects with impaired growth or GH disorders who were treated with Genotropin and whose legally acceptable representative (parent/guardian) consented to their participation. Such broad inclusion criteria, together with an open-label study design, are both typical for many postmarketing, observational surveillance studies and constitute the major strengths of KIGS. KIGS houses data on the largest cohort of pediatric patients ever treated with GH and for the longest duration of follow-up, and, as such, has contributed substantially to broadening current knowledge of the treatment of impaired growth and GH disorders in childhood. Over the years, KIGS data have complemented those obtained in smaller, shorter clinical trials with Genotropin and have been used to evaluate safety signals, to explore specific investigator-generated research questions, and to respond to numerous regulatory queries regarding the use of Genotropin.
As stated previously, the major objectives of KIGS were to monitor the long-term safety and efficacy of Genotropin as prescribed in routine clinical practice—more specifically, the pediatric treatment regimen employed—noting that neither the dosing nor schedule was driven by the study protocol but rather stemmed from the discretion of each treating physician-investigator. The underlying premise of KIGS was that documentation of everyday clinical practice in an unrestricted manner (using investigator-determined patient data extracted from medical records at routine visits) would provide opportunities to better understand treatment outcomes in unselected patient cohorts, to monitor the pattern of usage of Genotropin across different countries, and to more accurately assess treatment-regimen safety profiles as they might appear under "real-life" conditions.
The analysis of data originating from a real-world clinical practice setting is challenging and mandates the existence of precisely defined visit windows for time points used in analyses. Wide definitions of these windows may address the issue of data completeness—an important limitation of NI studies. As reporting was not driven by a stringent protocol and largely depended on investigators and their engagement, all information available in the KIGS database was included in relevant analyses. Of note, given the NI nature of the study and, as seen with similar studies, there is a potential bias due to underreporting of abnormal findings or AEs. Despite these limitations, however, the large number and broad characteristics of the pediatric cohorts, combined with their long-term followup, contribute greatly to the value of the data collected in KIGS.
KIMS
In 1994, KIGS spawned KIMS (Pfizer International Metabolic Database), a pharmaco-epidemiological registry aimed at assessing long-term clinical and safety outcomes of Genotropin treatment in adult patients with GH deficiency diagnosed either de novo in adulthood or previously during childhood [11]. The study, which lasted until 2012, enrolled 15,809 GH-treated adults (mean follow-up, 5.3 years) from 31 countries in 5 continents, with its key safety findings being that neither adultnor childhood-onset GHD was associated with increased de novo cancer risks or any clinically meaningful changes in lipids and fasting blood glucose [12].
Special aspects of KIGS
1. Growth-prediction models
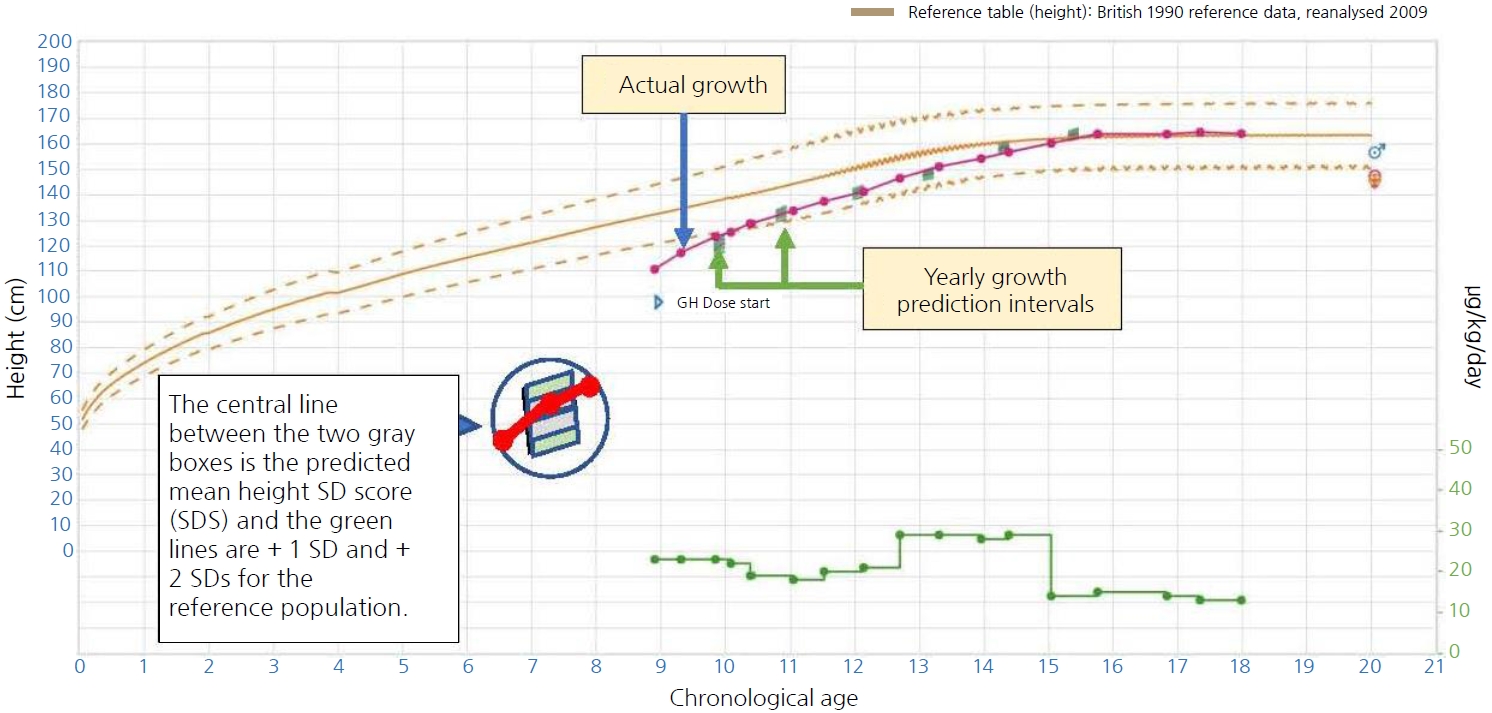
Using mathematical algorithms derived from (and subsequently validated by) KIGS data, growth-prediction models were developed under the leadership of Dr. Michael Ranke, with statistical support from Anders Lindberg, MS, from the SEC, for children treated with GH due to a number of indications in order to predict individual patient growth responses to treatment, based on a multivariate analysis of a number of relevant clinical characteristics, including firstyear height velocity on GH therapy, patient age, distance from current height to the genetic target height, body weight, birth weight, and GH dose (and, for children with GHD, its degree of severity) [13]. These algorithms could explain, with a low margin of error, a high degree of the observed variability of the response to GH during the first and subsequent prepubertal treatment years. During subsequent prepubertal years, weight, age, GH dose, and height gain during the previous year of GH treatment were the key predictors of future growth. The algorithm-generated predicted height velocity described the most likely growth pattern of an individual child, whereas a separate measure known as the studentized residual, analogous to a SDS, was derived as an index of a child's actual growth versus his or her unique predicted growth. This mathematical term, which can serve as an index of responsiveness to rhGH, is used in contrast to only evaluating a child's height in response to GH using growth charts or velocity targets. Models were developed and published for the following indications and described durations of therapy: (1) GHD, prepubertal years 1–8 of GH treatment; (2) TS, prepubertal years 1–8 of GH treatment; (3) SGA, prepubertal years 1 and 2 of GH treatment; and (4) ISS, prepubertal year 1 of GH treatment [14]. Subsequently, models were developed to predict pubertal growth in these 4 conditions [15].
To further support the clinical management of children treated with GH for GHD, TS, and short children born SGA, the aforementioned KIGS data were used to develop independent (stand-alone) cloud-based, accessible, easy-touse, clinically validated growth-prediction models (Fig. 1). Seventeen such models derived from the KIGS database were included and successfully tested for prediction accuracy and hardware/software compatibility. When the tool detected any discrepancies between the actual and predicted height, clinicians could investigate potential causes for such deviations and, hence, optimize the child’s GH treatment. It was important that the tool retained the critical features of the previous system, which forecasted growth before the start of GH treatment, providing both prepubertal and, in some cases, pubertal growth predictions, and that it presented a measure of individual responsiveness to rhGH. This tool, known as Individualised Growth Response Optimisation (iGRO), was designed to ensure compatibility with the majority of hardware/software platforms (desktops, laptops, and tablet devices) and web browsers. Throughout its development, access to iGRO was continually tested across a number of hospitals and clinics in Europe via the use of an active iGRO web link [16].
2. Project units
Project units using KIGS data to evaluate growth- and/or GH-specific questions were formed and composed of experts in the specific area culled from KIGS investigators. Among others, these included the KIGS Pharmacogenetics Project Unit (aimed at the identification of genes affecting height velocity during GH therapy and the use of this information to improve prediction models) and the KIGS Transition Project Unit (with the objective of studying patients with growth disorders receiving or not receiving GH therapy for 3 years following the attainment of adult height). In addition, combined KIGS/KIMS Project Units were also constructed as appropriate. One such area related to craniopharyngioma, and relevant studies covered changes in anthropometrics in children with craniopharyngioma after 3 years of GH therapy [17], baseline characteristics and response to 2 years of GH replacement in adult-onset craniopharyngiomas [18], clinical characteristics and effects of GH replacement therapy in adults with childhood-onset craniopharyngioma [19)], primary treatment regimen and diabetes insipidus as predictors of health outcomes in adults with childhood-onset craniopharyngioma [20], and contributing factors to morbidity and mortality in adults with craniopharyngioma on GH replacement [21].
3. Publications
1) Biannual reports
Biannual reports were a forum for formally publishing information of interest generated from KIGS that was not yet ready for inclusion of peer-reviewed articles due to a still-insufficient database and other aspects. As such, 24 KIGS Biannual Reports of the study progress were prepared during 1988–2009.
3) KIGS/KIMS expert meetings
The Expert Meetings and their resultant published Proceedings in Hormone Research are, in the opinion of the authors, the most remarkable activities related to the 2 databases covering a wide spectrum of topics and involving the greatest experts in the respective fields. In total, there were 10 such meetings, starting in 1995 (Table 4). The concept of the KIGS/KIMS Expert Meetings emanated from a goal to expand knowledge in the field of growth and GH therapy by providing a forum of discussion and debate to a group of experts from different expert backgrounds.
4) KIGS books
Three books (published after 5, 10, and 20 years of KIGS experience, respectively) including numerous articles from a great number of experts in the field of growth covered the state of GH therapy in children with short stature based on the experience accumulated from KIGS and other sources [23-25].
Conclusions
KIGS was an international, multicenter, NI study open to all pediatric subjects with various GH disorders who were treated with the Genotropin brand of rhGH. It is the largest, longest pharmaco-epidemiological study of GH usage in a real-world setting to date and found that rhGH is safe and increases both short-term height gain and adult height across multiple GHD and non-GHD conditions.